
Caregiver decision guide
Getting Started as a Family Caregiver: A Practical Guide for Adult Children
A foundational orientation guide for adult children who have recently stepped into a caregiving role for an aging parent — whether through gradual drift or sudden crisis — covering how to assess your parent's actual needs, secure critical legal access, build a support team, and protect your own health from day one.

You Are a Family Caregiver — and You Are Not Alone
Maybe it started with a phone call. Your mother fell and spent three days in the hospital. Or maybe it was slower — you noticed your father was letting bills pile up, skipping meals, losing track of his medications — and you quietly started filling in the gaps without ever naming what you were doing.
Either way, you are now a family caregiver. And you are in very large company.
According to the 2025 AARP and National Alliance for Caregiving national report, 63 million Americans — roughly 1 in 4 adults — are currently providing unpaid care to an aging family member. That number has grown by 45 percent over the past decade. The average caregiver is 51 years old. Three in five are women. Nearly a third are also raising children of their own.
If you feel underprepared, you are not behind. You are typical. The caregiving role is one that most people enter without a plan, without training, and without a clear sense of what it will actually require. This guide exists to give you the orientation that most caregivers never receive.
How People Become Family Caregivers
One of the most consistent findings in caregiving research is that most adult children do not recognize themselves as caregivers — even while they are actively providing care. This is not denial. It reflects how caregiving actually begins.
Research from the National Academies of Sciences, Engineering, and Medicine describes caregiving trajectories as moving through distinct phases: awareness, unfolding responsibility, and increasing care demands. Each phase looks different and requires different skills and resources.
- Gradual drift: You begin noticing small things — a parent struggling to balance a checkbook, forgetting appointments, letting the house go. You start helping with one task, then another, then several. The role accumulates before you name it.
- Crisis entry: A fall, a stroke, a dementia diagnosis, or another acute event suddenly makes caregiving visible and urgent. You are thrust into decisions and logistics with little time to orient yourself.
Both pathways are common and both are legitimate starting points. The research is clear that delayed self-identification as a caregiver is one of the main reasons people miss access to support programs, community resources, and peer networks that could reduce their burden significantly. Naming the role is the first practical step.
What Family Caregivers Actually Do: The Five Role Domains
The word "caregiver" can sound deceptively simple. In practice, the role spans five distinct domains, each with its own demands and skill requirements. Understanding these domains helps you recognize what you are already doing — and what you may need to prepare for.
- Household and personal care: Assistance with daily tasks including bathing, dressing, meal preparation, housekeeping, and mobility. This is often where caregiving begins and where it is most physically demanding.
- Emotional and social support: Providing companionship, managing anxiety or depression in the person receiving care, and maintaining their connection to social relationships and meaningful activities.
- Health and medical management: Administering medications, monitoring symptoms, coordinating follow-up care, communicating with physicians, and managing medical equipment. This domain has expanded significantly as hospital stays have shortened and more care has shifted into homes.
- Care coordination and advocacy: Navigating healthcare systems, scheduling and attending appointments, communicating across providers, and advocating for the care recipient's preferences and needs within medical and social service settings.
- Surrogate decision-making: Making medical, financial, and personal decisions on behalf of a parent who cannot make them independently — a responsibility that requires both legal authority and deep knowledge of the person's values and wishes.
What makes the medical management domain particularly significant is its complexity. According to the National Academies research, more than 60 percent of family caregivers manage medications on their own, and nearly half report receiving no training from any source before taking on these tasks. Older adults' homes have effectively become clinical care settings — and family members are the primary workforce.
Assessing Your Parent's Actual Needs: The ADL and IADL Framework
One of the most common mistakes new caregivers make is relying on intuition to gauge how much help a parent actually needs. Intuition tends to underestimate — especially for tasks that happen behind closed doors, like managing finances or taking medications correctly.
Healthcare providers use a structured framework to assess functional capacity: Activities of Daily Living (ADLs) and Instrumental Activities of Daily Living (IADLs). Understanding this framework gives you a more accurate picture of your parent's current situation and helps you communicate clearly with doctors, home care coordinators, and other members of your support team.
| Category | Specific Activities | Clinical Significance |
|---|---|---|
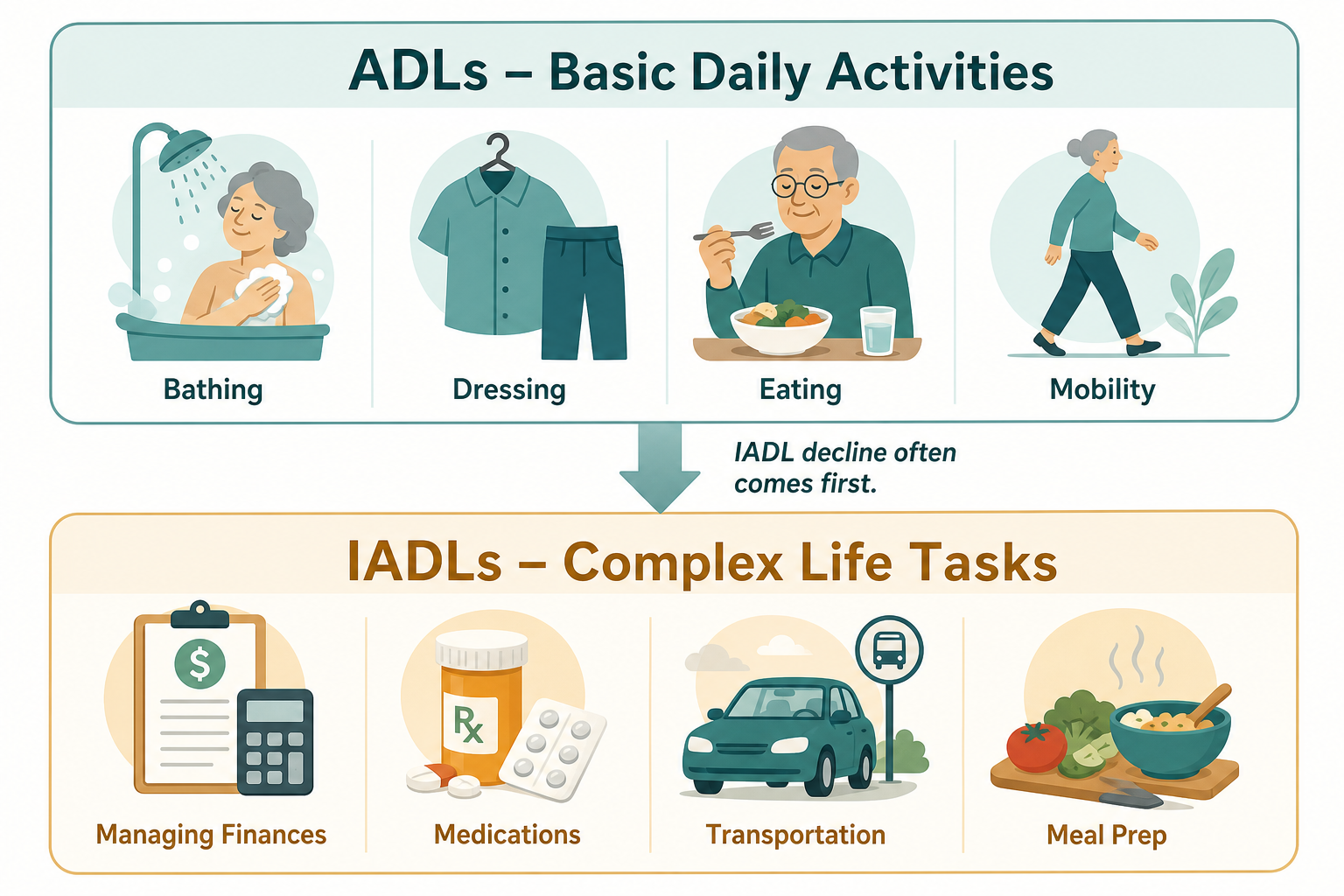
| Basic ADLs | Bathing, dressing, eating, toileting, transferring (moving from bed to chair), continence | Difficulty here signals significant functional decline; often triggers eligibility for intensive home care or facility-level care |
| Instrumental ADLs (IADLs) | Managing finances, medications, transportation, meal preparation, housekeeping, communication devices | IADL decline typically precedes ADL decline and is frequently missed; drives eligibility for adult day programs, paid home care, and assisted living |
The clinical insight most relevant to family caregivers: IADL decline almost always comes first. A parent who is managing their own bathing and dressing may already be struggling significantly with finances, medications, or meal planning — and may not volunteer that information. Asking directly about IADL tasks, or observing them in context, gives you a more accurate baseline than asking "how are you doing?"
Clinicians use two standardized tools for formal assessment: the Katz Index of Independence in ADL for basic activities, and the Lawton Instrumental ADL Scale for instrumental activities. You do not administer these yourself — they are clinical instruments — but knowing their names helps you ask informed questions during your parent's medical appointments and understand what assessments have or have not been completed.
Securing Your Legal and Medical Foundation Before You Need It
There is a narrow window in which these documents can be executed — and most families do not realize how narrow it is until it has closed.
Legal documents that authorize a family caregiver to act on a parent's behalf — in medical settings, financial institutions, and emergency situations — can only be signed by someone with legal and cognitive capacity to do so. Once a parent has experienced significant cognitive decline, a stroke, or another incapacitating event, the window closes. At that point, obtaining legal authority often requires a court-supervised guardianship or conservatorship process that is far more costly, time-consuming, and emotionally difficult than executing documents in advance.
The stakes are concrete: family members are involved in medical decisions for nearly 47 percent of hospitalized older adults, including 23 percent who need all decisions made by a surrogate. Without legal documentation in place, your ability to act — to access medical records, speak with physicians, make financial decisions, or authorize treatment — may be blocked at precisely the moment you most need it.
- Healthcare power of attorney (HCPOA): Designates who can make medical decisions if your parent cannot make them. Without this document, hospitals may be legally prevented from sharing information with you or following your guidance.
- Financial power of attorney (FPOA): Authorizes you to manage financial accounts, pay bills, handle property, and make financial decisions on your parent's behalf. Scope and limitations vary by state.
- HIPAA authorization: A separate, often-overlooked document that explicitly permits healthcare providers to share medical information with you. Even with an HCPOA in place, some providers will request a HIPAA release before discussing a patient's care.
- Advance directive (living will): Documents your parent's wishes regarding end-of-life treatment, resuscitation, and life-sustaining measures. Reduces the burden on you to make these decisions under pressure and ensures your parent's preferences are honored.
In addition to legal documents, gather practical information now: a current medication list with dosages, names of all treating physicians and their contact information, insurance cards and policy numbers, and the location of important documents including the will, insurance policies, and financial account information. The time to organize this is before a crisis makes it urgent.
Building Your Care Team: Caregiving Is Not a Solo Journey
The image of a single adult child managing everything alone — the appointments, the medications, the household, the emotional labor — is common. It is also a path toward exhaustion. Building a care team is not a sign that you cannot handle caregiving. It is what sustainable caregiving actually looks like.
A realistic care team has four layers:
- Family coordination: Dividing tasks among siblings or other family members based on availability, geography, and individual strengths — not guilt or birth order. A sibling who lives far away may handle financial management and insurance coordination; one who lives nearby may handle transportation and appointments. Making these divisions explicit reduces resentment and gaps.
- Community and government resources: Every county in the United States has an Area Agency on Aging (AAA), which connects caregivers to local services including meal delivery, transportation, respite care, caregiver support groups, and benefits counseling. PACE programs (Program of All-Inclusive Care for the Elderly) provide comprehensive services for eligible older adults who qualify. Veterans and their spouses may have access to VA caregiver support programs. These resources exist specifically for families in your situation.
- Professional home care: Paid care workers range from companion care (non-medical support with daily tasks and companionship) to home health aides (personal care assistance) to skilled home health nursing (medical care ordered by a physician). Understanding these distinctions helps you identify what level of professional support is appropriate for your parent's current needs.
- Peer support: Caregiver support groups — available through hospitals, faith communities, disease-specific organizations, and online — connect you with people who understand the experience from the inside. The practical knowledge and emotional validation that come from peer support are not available anywhere else.
Protecting Yourself: Caregiver Wellbeing Starts on Day One
This section is not optional reading. It is not a gentle reminder to "take care of yourself." It is a clinical reality that the caregiving literature is unambiguous about: caregivers who neglect their own health become less capable caregivers, and eventually become unable to provide care at all.
The numbers from a 2026 survey of more than 1,000 family caregivers are stark: 42 percent experience emotional burnout at least weekly. Nearly half — 47 percent — report that their physical health has declined since taking on caregiving responsibilities. Three-quarters feel stressed or anxious at least monthly. More than 7 in 10 report feeling overwhelmed.
These are not outliers. They are the norm. And they are significantly more likely when caregivers do not establish boundaries, build support systems, and monitor their own wellbeing from the beginning of the caregiving journey — not after they have already hit a wall.
Early Warning Signs of Caregiver Burnout
Burnout rarely announces itself clearly. It tends to accumulate through symptoms that are easy to rationalize as temporary stress:
- Persistent exhaustion that sleep does not resolve
- Increasing irritability or resentment toward the person you are caring for
- Withdrawing from relationships, activities, or interests you previously valued
- Neglecting your own medical appointments, medications, or basic self-care
- Feeling that caregiving has consumed your identity — that you have no role outside of it
- Using alcohol, food, or other substances to manage stress
- Persistent feelings of hopelessness or inability to imagine the situation improving
If several of these feel familiar, you are not failing. You are experiencing what the research predicts for caregivers who carry the role without adequate support. The appropriate response is to treat this as information — and to take concrete steps to rebuild your support structure.
The Sandwich Generation Reality
If you are also raising children, the compounded demands are not a personal failure of time management. According to the 2025 AARP/NAC report, 29 percent of all caregivers — and 47 percent of those under age 50 — are simultaneously caring for both an aging parent and dependent children. The financial and emotional strain of this position is well-documented and significant.
Your Caregiving Learning Path: What to Explore Next
This guide covers the foundational orientation that every family caregiver needs. As your caregiving situation develops, you will encounter more specific questions — about your parent's home safety, their medical condition, the technology that can support them, and the legal and financial decisions ahead. The following areas of this site are organized to meet those needs as they arise.
- Fall Prevention: Falls are the leading cause of injury among older adults and one of the most common triggers for caregiving crises. The fall prevention guides here are organized by room and use the CDC STEADI framework to help you assess and address hazards systematically — from the bathroom to the staircase to the entryway.
- Memory Care: If your parent has received a dementia diagnosis — or if you are observing cognitive changes that concern you — the memory care section provides stage-specific guidance and behavior reference pages for specific symptoms including wandering, sundowning, and agitation.
- Aging-in-Place Home Modifications: Structural changes to the home — grab bars, ramps, wider doorways, improved lighting — can significantly extend your parent's ability to remain safely at home. This section covers modification types by room, cost ranges, and funding sources including VA grants and Medicaid waivers.
- Senior Monitoring Technology: Personal emergency response systems, GPS trackers, passive home sensors, and wearable health monitors are among the technology categories that support aging at home. The monitoring technology guides here are product-neutral — they explain how each category works and what to evaluate, without recommending specific brands.
- Mobility and Daily Independence: Walkers, rollators, canes, transfer aids, shower chairs — understanding which mobility aids match which functional needs helps you make informed decisions alongside your parent's occupational or physical therapist.
- Caregiver Wellbeing: The wellbeing section is a parallel track dedicated to your own health and sustainability — covering burnout recognition, respite care options, caregiver guilt, and how to approach difficult conversations with your parent about accepting help, stopping driving, or transitioning to a higher level of care.
You do not need to read all of this at once. Return to it as your situation evolves. The caregiving journey is rarely linear, and the most useful guides are often the ones you find six months from now — when a new challenge has emerged and you need a reliable place to start.
Questions to bring to a clinician or OT
This is not medical, legal, or a family's final decision — only a framework. Bring these questions to a clinician, occupational therapist, or your local Area Agency on Aging.
Find Local HelpRelated reading
Noticed something outdated or inaccurate on this page? Flag a correction. We review every report against CDC, NIA, and AARP HomeFit guidance before updating a page.