
Caregiver decision guide
Medication Management for Older Adults: A Caregiver's Practical Guide
Most family caregivers take on medication management for an older adult without any training — this guide walks you through building a master medication list, organizing a safe home system, recognizing dangerous drug interactions, navigating dementia-specific challenges, and protecting your loved one at high-risk care transitions like hospital discharge.

Why Medication Management Falls to Family Caregivers — and How Unprepared Most Are
When a parent comes home from the hospital with a bag full of new prescriptions, or a spouse's health conditions multiply over the years, medication management rarely gets handed off with any formal training. It simply becomes part of the job — and most caregivers figure it out as they go.
Research confirms how common and how unsupported this role is. Medication management is the most common medical task performed by informal caregivers, with 78% managing a loved one's medications. More than half administer five or more different prescription medications daily. Nearly one in five administer ten or more. And the majority of these caregivers learn entirely on their own — nearly half never receive training from any source.
The stakes of getting this wrong are real. Older adults visit emergency departments more than 600,000 times each year for adverse drug events — more than twice the rate of younger adults. Medications that are poorly organized, missed, doubled up, or combined dangerously are a leading cause of those visits.
This guide offers the structured framework most caregivers never receive. It covers every stage of the medication management role: building a reliable medication record, organizing a safe home system, understanding the risks of polypharmacy, supporting adherence, managing dementia-specific challenges, recognizing warning signs, and protecting your loved one at the highest-risk moments — including hospital discharge.
Building the Master Medication List
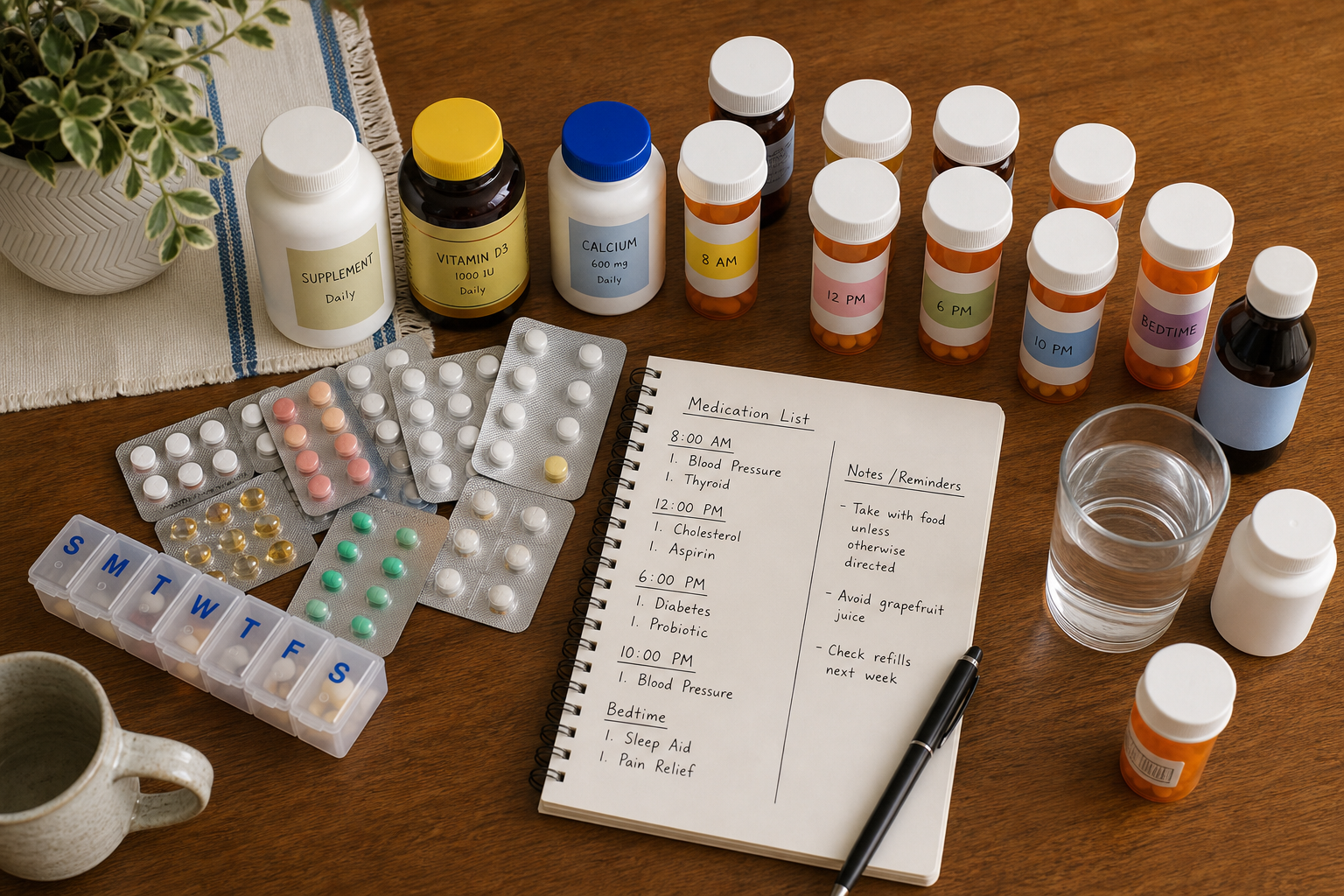
The single most important tool in medication management is a complete, current, written medication list. Every other system — pill boxes, reminders, care-transition checklists — depends on this foundation being accurate.
The FDA recommends maintaining a written list of all medications — including over-the-counter drugs, vitamins, and dietary supplements — with specific details for each. The Family Caregiver Alliance reinforces this, noting the list should be kept current and shown to every healthcare provider, including dentists and physical therapists.
For each medication on the list, capture the following:
| Field | What to Record | Why It Matters |
|---|---|---|
| Drug name | Both generic name and brand name | Prevents accidental duplication when a refill comes with a different label |
| Dose | Exact amount per dose (e.g., 10 mg) | Catches dose discrepancies across prescribers |
| Frequency and timing | How many times per day and when (e.g., with breakfast, at bedtime) | Supports consistent adherence and avoids missed or doubled doses |
| Administration instructions | With food, with water, swallow whole, sublingual, etc. | Some instructions affect absorption and safety |
| Indication | What condition or symptom this medication treats | Helps identify when a drug may no longer be needed |
| Prescribing provider | Name and contact of the prescriber | Essential at transitions and when questions arise |
| Known side effects | Common and serious side effects to watch for | Helps caregivers recognize adverse events early |
| OTC drugs, vitamins, supplements, herbals | Include everything taken regularly | Herbals and supplements carry interaction risks and are not interchangeable with prescription drugs in terms of safety assumptions |
Keep both a paper copy and a digital backup. The paper copy travels to appointments; the digital backup can be updated quickly and shared with other family members or providers. Review and update the list after every appointment, prescription change, or care transition.
Organizing Medications at Home: Matching Tools to Your Loved One's Needs
The right organizational tool depends on the person — their cognitive status, physical dexterity, and the complexity of their regimen. What works well for a cognitively intact older adult managing two daily medications may fail completely for someone with early dementia managing eight.
Pill Boxes and Manual Organizers
Pill boxes are the most widely used medication organization tool. When evaluating options, consider these dimensions rather than defaulting to the most familiar format:
- Compartment size: Large enough for the person's hand strength and dexterity to open reliably
- Time slots: Single daily compartment vs. multiple slots per day (AM/PM, four times daily) depending on dosing schedule
- Detachable day sections: Allow a single day's medications to be separated and carried, reducing the chance of taking the wrong day's dose
- Locking mechanisms: Essential when the care recipient has dementia and should not have unsupervised access to a week's supply of medications
- Weekly vs. monthly format: Weekly batch preparation is manageable for most caregivers; monthly formats work for simpler regimens
Labeling and color-coding can supplement the pill box — color-coded dots on prescription bottles that correspond to the time of day they are taken help reduce confusion during administration. Some caregivers use separate cups or plates as visual cues at the table to signal that it is medication time.
Automatic Pill Dispensers
When a simple pill box is not sufficient — because the care recipient forgets to take medications, takes the wrong compartment, or should not have access to a full week's supply — automatic dispensers offer a meaningful step up. Evaluate these category-level dimensions when comparing options:
- Locking mechanisms that prevent access to medications outside of scheduled dose times
- Dose capacity — how many days or doses can be loaded at once before the caregiver needs to refill
- Caregiver alert capability — whether the device notifies a caregiver remotely when a dose is missed
- Connectivity — whether alerts arrive by phone call, text, or app, and whether that matches how the caregiver is reachable
- Audible and visual alerts for the care recipient at dose time
Restricting Access for Dementia
As dementia progresses, independent access to medications becomes a safety risk — not just a reliability concern. A person with moderate to severe dementia may take the same medication twice, refuse a dose, or take medications belonging to someone else. Storing medications out of reach, in a locked cabinet, or in a locking dispenser is not about distrust — it is a straightforward safety measure that becomes necessary as cognition declines.
Establishing Adherence Routines and Reminder Systems
Consistent medication-taking is easier to sustain when it is anchored to existing daily routines rather than treated as a separate task. Linking a morning medication to breakfast, or a bedtime medication to tooth-brushing, reduces the cognitive load of remembering and makes adherence feel automatic rather than effortful.
Beyond routine anchoring, caregivers use a range of reminder strategies. The right combination depends on the care recipient's preferences and cognitive status:
- Alarm-based reminders: Phone alarms, clock radios, or dedicated medication reminder devices set to dose times
- Visual cues: Sticky notes on the refrigerator, a whiteboard in the kitchen, or a calendar with medication times marked
- The filled pill box as a visual check: An empty compartment confirms the dose was taken; a full compartment signals it was not
- Apps and subscription reminder services: Useful for caregivers managing their own reminders to administer or check on medications
- Verbal reminders: Effective for many older adults, but the approach matters — see below
Patient autonomy is a real dimension of medication adherence. Research on caregiver involvement in medication management identifies a common pattern: the caregiver perceives a need to help, offers assistance, and the older adult rejects it — leaving the caregiver to monitor from a distance without being able to intervene directly. This 'peripherally involved' scenario is the most emotionally challenging for caregivers.
When a loved one resists direct reminders — particularly if they feel their independence is being questioned — indirect approaches can reduce friction. Framing a reminder as part of a shared routine ('I'm making coffee, want to take your morning pills with me?') is often more effective than a direct prompt. Respecting independence where it is safe to do so, and escalating concerns to the care team when it is not, is the right balance.
Understanding Polypharmacy and the Beers Criteria: What Caregivers Need to Know
Polypharmacy — the use of multiple medications simultaneously — is not an edge case in older adult care. It is the norm. Approximately 40% of adults 65 and older take five or more prescription medications to manage multiple chronic conditions. Polypharmacy is generally defined as five or more medications at discharge from a hospital, or ten or more during hospitalization.
The risks compound quickly. Each additional medication increases the potential for harmful drug interactions. More broadly, polypharmacy is an independent risk factor for falls, cognitive impairment, delirium, hip fractures, hospitalization, and long-term care placement. It also contributes to a pattern called the prescribing cascade.
A prescribing cascade begins when a drug side effect is misinterpreted as a new medical condition. A provider prescribes an additional medication to treat what appears to be a new symptom. That medication causes its own side effect, which is again misread as a new condition — and the cycle continues. Recognizing this pattern is one of the most valuable things a caregiver can do.
High-Risk Drug Classes in Older Adults
The American Geriatrics Society publishes the Beers Criteria — an evidence-based list of medications that are potentially inappropriate for older adults. Caregivers can use this as an advocacy reference when speaking with providers, not as a self-administered screening tool.
| Drug Class | Examples of Concerns in Older Adults |
|---|---|
| Anticholinergics | Delirium, memory loss, hallucinations, falls, urinary retention |
| Sedatives and benzodiazepines | Confusion, falls, respiratory depression, dependence |
| First-generation antihistamines | Sedation, anticholinergic effects, confusion (e.g., diphenhydramine in many sleep aids) |
| Certain NSAIDs | Renal failure, gastrointestinal bleeding, fluid retention |
| Long-acting sulfonylureas | Prolonged hypoglycemia risk |
| Certain cardiovascular agents | Hypotension, dizziness, fall risk |
| Narcotics / opioids | Dependency, confusion, falls, respiratory depression |
Pharmacist-led medication reviews have been shown to meaningfully reduce polypharmacy. Research cited in the StatPearls polypharmacy review found a 67% reduction in polypharmacy after the first pharmacist intervention. If your loved one's regimen feels unwieldy, requesting a formal medication review — or a 'brown bag' review where all medications are brought to the pharmacist at once — is a concrete next step.
Managing Medications When Your Loved One Has Dementia
Dementia changes medication management in ways that most general caregiver guides do not address. As cognition declines, the responsibility for medication management transfers progressively from the person to the caregiver — but this transfer is rarely smooth or linear.
A systematic review of medication management in dementia identified four domains that shape how medications are managed as the disease progresses: cognitive challenges (impaired planning, forgetfulness, lack of insight into the need for medication), medication-related factors (supply logistics, administration complexity, safety), social and practical factors (caregiver availability and stress), and knowledge and communication barriers (difficulty understanding regimens, making clinical judgments).
Medication Refusal
In middle and later stages of dementia, medication refusal is common. It can take the form of suspicious thinking ('You're trying to poison me'), anger, flat denial, or simply spitting out pills. This is not willfulness — it reflects the disease's effect on insight and trust.
Strategies that caregivers have found effective include:
- Calm, unhurried repetition without arguing about whether the medication is needed
- Embedding medication administration in a familiar routine (after breakfast, during a regular activity) so it feels like a normal part of the day
- Using indirect reminders rather than direct commands, which can trigger resistance
- Offering a small amount of a preferred food or drink alongside the medication to make administration feel less clinical
- Concealing medication in food — only when clinically appropriate and only after discussing this approach with the prescriber, as some medications must not be crushed or mixed
When refusal is persistent or escalating, this is a clinical conversation — not a caregiver problem to solve alone. Bring it to the prescriber. In some cases, the medication may need to be reformulated, substituted, or reconsidered. In late-stage dementia, persistent refusal may require a different care approach altogether.
The emotional burden of this role is real. Being responsible for a loved one's medications while simultaneously managing their resistance, their safety, and your own uncertainty is one of the most demanding aspects of dementia caregiving. Acknowledging that burden — rather than treating it as a logistics problem — is part of sustaining the caregiver role over time.
Recognizing Adverse Drug Events and Dangerous Interactions
One of the most practical principles in geriatric pharmacology is this: any new symptom in an older adult should be treated as a possible drug side effect until proved otherwise. The Family Caregiver Alliance's guide to medications and aging frames this explicitly: caregivers who internalize this principle are better positioned to catch adverse drug events before they become emergencies.
Red-flag symptoms that may signal a medication-related problem include:
- Excessive drowsiness or sedation that is new or worsening
- Confusion, disorientation, or delirium
- Depression or significant mood change
- Parkinson's-like symptoms: tremor, shuffling gait, muscle stiffness
- New or worsening incontinence
- Unexplained falls or balance problems
- Loss of appetite or significant weight loss
- Memory changes or cognitive decline that appears abruptly
- Changes in speech, coordination, or muscle control
Drug-drug interactions are one common cause of these symptoms, but environmental interactions matter too. Grapefruit juice, for example, can significantly affect how certain medications are metabolized — including some statins, calcium channel blockers, and immunosuppressants. Alcohol interacts dangerously with sedatives, blood thinners, and many other drug classes.
Watch for the prescribing cascade pattern: if a provider prescribes a new medication shortly after a new symptom appears, it is reasonable to ask whether the new symptom might be a side effect of an existing medication rather than a new condition requiring treatment.
Medication Safety at Care Transitions: What to Do at Hospital Discharge
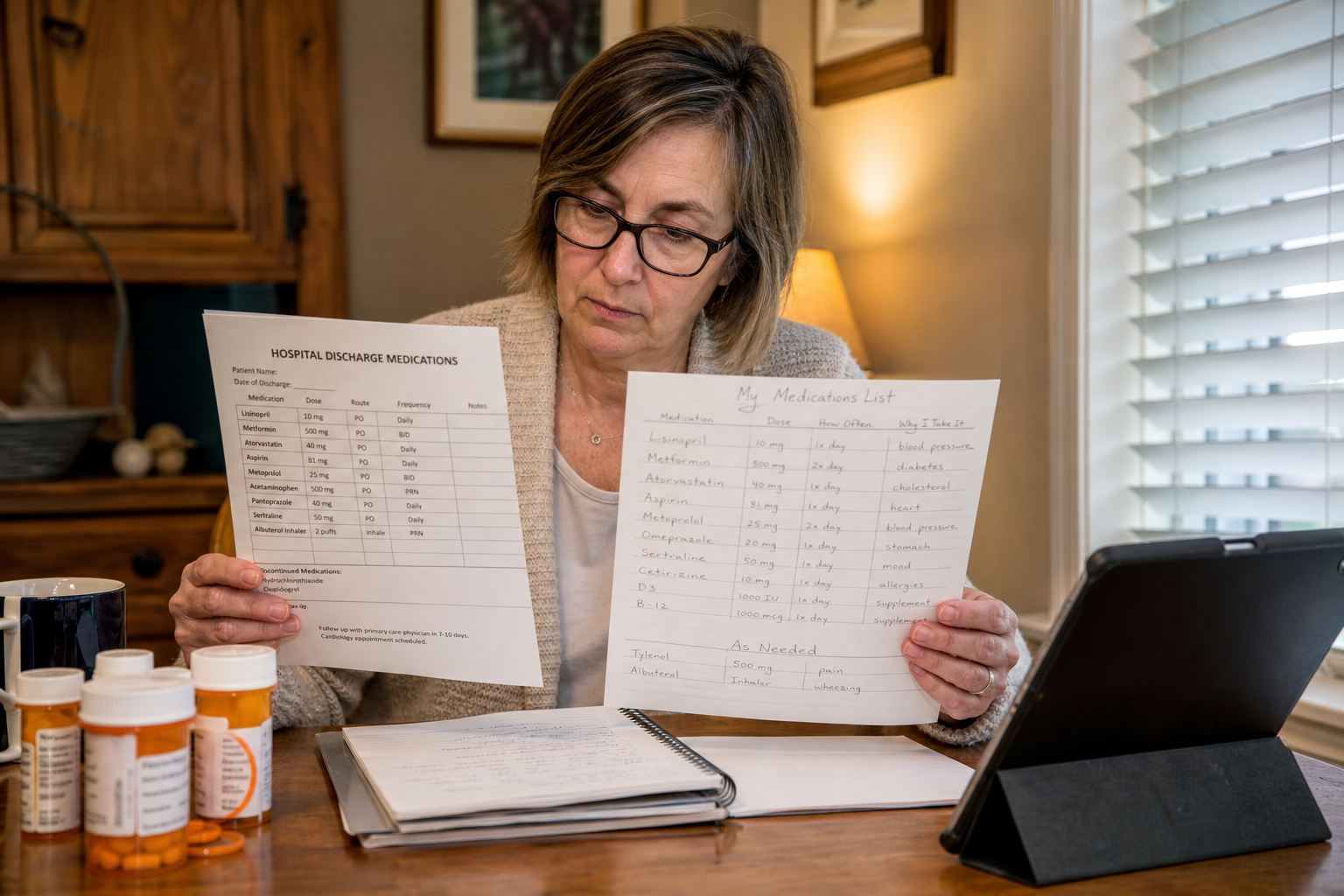
Hospital discharge is the highest-risk moment for medication errors in older adult care. Multiple prescribers, partial or outdated information, and inadequate discharge training create conditions where mistakes are common. Issues with prescription medications most commonly emerge at transition points — specialist referrals and hospital discharges — where poor coordination causes providers to update medications based on partial or outdated information.
Research confirms that caregivers frequently receive inadequate training at discharge. The medication list handed to a caregiver at discharge may include new medications, discontinued medications, dose changes, and medications that were paused during the hospital stay — without clear explanation of what changed and why.
Before leaving the facility, work through a medication reconciliation process:
| Step | What to Do | Questions to Ask |
|---|---|---|
| Compare lists | Place the discharge medication list next to the home medication list and compare them side by side | Which medications are new? Which were stopped? Which doses changed? |
| Identify new medications | For each new drug, confirm the indication, dose, duration, and expected side effects | Why was this prescribed? How long will my loved one take it? What should I watch for? |
| Identify discontinued medications | Confirm which home medications were stopped and whether the stop is permanent or temporary | Is this medication stopped permanently, or just while they recover? |
| Confirm dose changes | Note any medications where the dose changed from the home regimen | Why was the dose changed? Should I use the old supply or get a new prescription? |
| Clarify timing | Confirm whether any medications have new timing instructions (e.g., with food, at a different time of day) | Are there any new administration instructions I need to know? |
| Ask about follow-up | Confirm which medications need lab monitoring and when the first follow-up appointment should occur | When should I have blood work done for this new medication? |
Partnering with the Pharmacist and Healthcare Team
The pharmacist is the most underused partner in family caregiving. Most caregivers interact with the pharmacist only at the prescription counter — but pharmacists offer a range of services that can meaningfully reduce medication complexity and risk.
Services available through many community pharmacists include:
- Medication therapy management (MTM): A structured review of all medications to identify interactions, duplications, and opportunities to simplify the regimen — often covered by Medicare Part D for eligible patients
- Brown bag medication review: Bring all medications to the pharmacy at once for a comprehensive review; no appointment needed at many pharmacies
- Large-print labels: Available on request for older adults with vision impairment
- Tablet splitting: For medications where splitting is clinically appropriate, pharmacists can advise on technique and provide pill splitters
- Instruction on injectable or inhaled medications: Particularly valuable after discharge when new delivery methods are introduced
- Pill box matching: Pharmacists can recommend organizer types suited to the individual's dexterity, regimen complexity, and cognitive status
Coordinating across multiple prescribers is one of the most common sources of medication risk. Every provider — not just the primary care physician, but also specialists, dentists, and physical therapists — should receive a current copy of the master medication list at every visit. When a new prescription is written, ask the prescriber to check for interactions with the existing regimen, and confirm the same with the dispensing pharmacist.
Safe Storage, Disposal, and Travel
Storage
Most medications should be stored in a cool, dry location — not the bathroom medicine cabinet (humidity degrades many drugs) and not near the stove or kitchen window (heat accelerates breakdown). The FDA recommends keeping medications out of reach of children; for households where someone with dementia lives, medications should also be inaccessible to the care recipient unless supervised.
Check expiration dates periodically. Expired medications may be less effective or, in some cases, chemically altered. Discard them promptly using a safe disposal method.
Disposal
Do not flush unused medications down the toilet or throw them in the household trash unless the FDA specifically lists them as safe to flush. The preferred method is an FDA-approved drug take-back program. Many pharmacies and law enforcement agencies host take-back collection sites. The DEA's National Prescription Drug Take Back Day occurs twice annually and provides convenient community drop-off locations.
Travel
- Keep medications in their original labeled containers when traveling — unlabeled pills can create problems at security checkpoints and in emergencies
- Carry a copy of the master medication list in your travel bag, separate from the medications themselves
- For time-sensitive medications, plan ahead for time-zone changes — ask the prescriber or pharmacist how to adjust timing across time zones
- Bring enough supply for the full trip plus a buffer of several days in case of travel delays
- For medications requiring refrigeration, confirm storage requirements and plan accordingly before departure
Resources for Caregivers Managing Medications
The following authoritative resources offer additional guidance for caregivers managing an older adult's medications:
- National Institute on Aging (NIA): Guidance on taking medicines safely as you age, including information on how aging affects drug metabolism and what to discuss with your provider.
- U.S. Food and Drug Administration (FDA): Medication safety tips for older adults and a drug take-back locator to find safe disposal sites near you.
- Centers for Disease Control and Prevention (CDC) — Medication Safety: Data on adverse drug events, emergency department visits, and medication safety statistics for older adults.
- American Geriatrics Society Beers Criteria: The evidence-based list of potentially inappropriate medications for older adults, updated regularly. Useful as an advocacy reference when speaking with prescribers.
- Family Caregiver Alliance — Caregiver's Guide to Medications and Aging: A pharmacist-authored overview of medication safety for caregivers, including red-flag symptoms, storage guidance, and questions to ask providers.
- Caregiver Action Network — Medication Guide: A downloadable caregiver medication guide with sections for medication records, side effects, immunizations, adverse reactions, and medical team contacts.
Questions to bring to a clinician or OT
This is not medical, legal, or a family's final decision — only a framework. Bring these questions to a clinician, occupational therapist, or your local Area Agency on Aging.
Find Local HelpRelated reading
Noticed something outdated or inaccurate on this page? Flag a correction. We review every report against CDC, NIA, and AARP HomeFit guidance before updating a page.