
Clinical term
ADL and IADL Decline Timeline: What Family Caregivers Should Expect
What Are ADLs and IADLs?
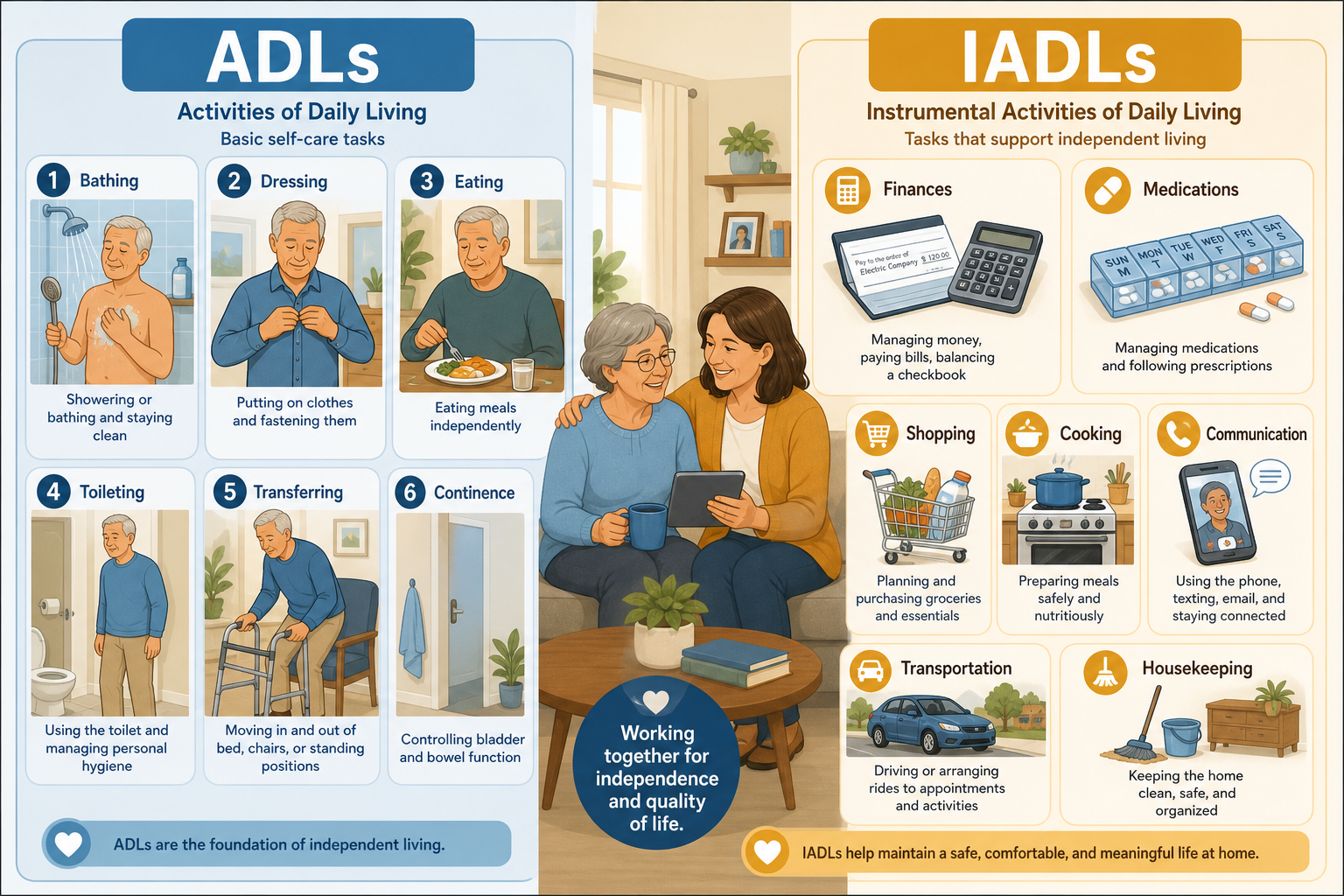
Activities of daily living (ADLs) and instrumental activities of daily living (IADLs) are two categories of tasks that clinicians and caregivers use to measure a person’s functional independence. The distinction matters because each set relies on different skills and tends to decline at different points along the aging and disease trajectory.
Basic ADLs, first defined by geriatrician Sidney Katz in the 1950s, are the fundamental self-care tasks needed to live independently at a physical level. The Katz Index evaluates six ADLs: bathing, dressing, toileting, transferring, continence, and feeding. IADLs, introduced by psychologist M.P. Lawton roughly a decade later, are more complex activities that require planning, judgment, and executive function — managing money, handling medications, using transportation, shopping, preparing meals, doing housework, doing laundry, and using a telephone.
| Category | Tasks | Required Cognitive Demand | Typical Order of Decline |
|---|---|---|---|
| Basic ADLs | Bathing, dressing, toileting, transferring, continence, feeding | Lower — primarily motor and procedural memory | Decline later, usually after significant brain or physical change |
| Instrumental ADLs (IADLs) | Managing finances, managing medications, using transportation, shopping, meal preparation, housekeeping, laundry, telephone use | High — requires executive function, working memory, planning, problem solving | Decline first, often the earliest sign of cognitive impairment |
Healthcare providers routinely assess both ADLs and IADLs when evaluating older adults with neurodegenerative disorders, according to Cleveland Clinic. The Lawton Scale covers eight IADL domains and is the most widely used instrument for measuring higher-level function. Understanding which tasks fall into each bucket helps caregivers spot early warning signs before a crisis emerges.
The Typical Decline Pattern: IADLs First, ADLs Later
For most older adults who develop Alzheimer’s disease or a related dementia, functional decline follows a predictable sequence: difficulties with IADLs appear months to years before basic ADLs are affected. Better Health While Aging notes this pattern is so consistent that IADL trouble is often the earliest detectable functional change in dementia and mild cognitive impairment. The StatPearls review confirms that "as individuals age and their functional status declines, they often need assistance with instrumental ADLs before requiring assistance with basic ADLs."
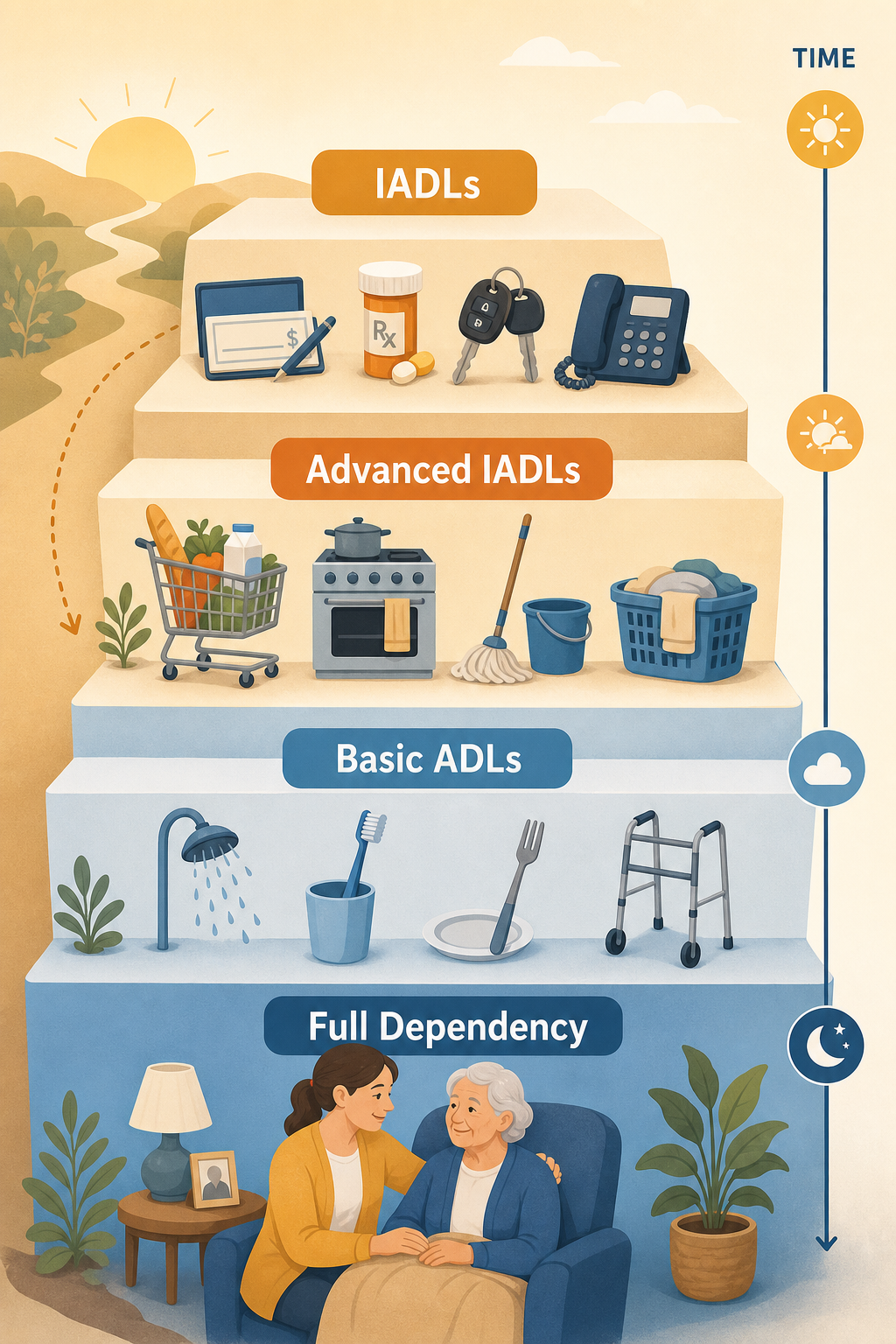
The trajectory can be mapped along a series of milestones:
- Early IADL loss — forgetting to pay bills, missing medication doses, getting lost while driving, neglecting meal preparation.
- Advanced IADL loss — unable to shop independently, stop cooking safely, needing help with housekeeping and laundry.
- Emerging ADL dependence — requiring prompting or assistance with bathing, dressing, or toileting.
- Full ADL dependency — requiring hands-on help with eating, transferring, and continence management.
This progression does not happen overnight. For some, it unfolds over years; for others, a sudden event like a hip fracture can cause a catastrophic drop in function across multiple domains. A 2020 systematic review of ADL and IADL assessment tools identifies two distinct pathways to disability: catastrophic (e.g., fracture or stroke) and progressive (gradual decline in brain function). Knowing which pattern is at play helps caregivers tailor their response.
Why IADLs Are Especially Sensitive to Early Cognitive Changes
IADLs are essentially real-world tests of executive function. The same cognitive abilities that allow us to plan a week of meals, track a checking account, or remember a medication schedule are the ones most vulnerable to early neurodegenerative changes. According to the PMC systematic review, "doing day-to-day functions, especially IADLs, has a significant correlation with executive functions such as planning, working memory, attention, problem solving, verbal reasoning and mental flexibility."
The eight Lawton IADL domains map directly to cognitive skills that decline early:
- Finances — requires calculation, judgment, and memory of recent transactions.
- Medications — requires memory of schedule, ability to read labels, and understanding of dosage.
- Transportation — requires spatial navigation, route planning, and quick decision making.
- Shopping — requires list planning, budgeting, and navigation of a complex environment.
- Meal preparation — requires sequencing, safety awareness, and multitasking.
- Housekeeping and laundry — require organizing, attention to detail, and initiation.
- Telephone use — requires recall of numbers, communication skills, and troubleshooting.
This connection is why a family member might notice mom's checkbook hasn't been balanced in months long before she struggles to button her shirt. The cognitive demand of IADLs acts as an early indicator, giving families a window of opportunity to put supports in place while basic self-care is still intact.
How Dementia and Frailty Patterns Differ
Not all functional decline follows the same script. The underlying cause — Alzheimer’s disease, vascular dementia, or physical frailty — shapes the order and speed of IADL and ADL loss. Understanding these differences helps caregivers anticipate what to expect and plan accordingly.
| Condition | Typical Decline Pattern | Key Features |
|---|---|---|
| Alzheimer’s disease | IADLs first (months to years), then gradual ADL decline | Progressive, predictable; executive function loss early; procedural memory preserved longer |
| Vascular dementia | Stepwise decline; can lose IADL and ADL function abruptly after each stroke | Sudden drops followed by plateaus; pattern varies by brain region affected |
| Frailty / musculoskeletal conditions | ADLs may decline first (mobility, bathing, transferring) while IADLs remain intact | Physical limitation precedes cognitive decline; IADLs may be preserved unless caregiver steps in |
| Mixed dementia | Combined pattern; IADL loss early but with physical components | Both cognitive and physical contributors; requires dual-track planning |
The StatPearls article categorizes ADL decline causes as catastrophic (e.g., hip fracture, stroke) or progressive (gradual brain function decline). In catastrophic cases, a person may go from independent to needing help with multiple ADLs almost overnight. Families then must respond quickly, often while still in shock. Conversely, progressive decline allows more time for planning — but the gradual erosion can sometimes go unnoticed until a crisis occurs.
Planning Care at Each Stage of Decline
The staged nature of functional decline creates clear opportunities to introduce support incrementally. Trying to add too much help too early can feel overwhelming or intrusive; waiting too long forces crisis-driven decisions. Matching the care level to the current stage of IADL/ADL loss keeps the older adult as independent as possible while preventing safety failures.
Below is a stage-by-stage guide based on the typical progression:
| Stage | Functional Signs | Recommended Supports | Setting Options |
|---|---|---|---|
| Early IADL loss | Forgets bills, misses meds, stops cooking, avoids driving | Medication organizer, automatic bill pay, meal delivery service, ride-sharing accounts | Home with family check-ins; possible home health aide for IADL support |
| Advanced IADL loss | Cannot shop alone, stops housekeeping, needs help with laundry | In-home caregiver (part-time), grocery delivery, housekeeping service, medication management | Home with paid caregiver or adult day program |
| ADL dependence (1–2 ADLs) | Needs help with bathing or dressing; occasional incontinence | Personal care aide (daily), grab bars and transfer aids, incontinence products | Home with live-in care; assisted living or memory care (if dementia) |
| Full ADL dependency | Needs hands-on help with eating, toileting, transferring; frequent incontinence | Skilled nursing: 24/7 care, feeding assistance, incontinence management, medication monitoring | Skilled nursing facility (SNF); hospice if end-stage |
When considering residential care, it helps to know what services are commonly available. A Place for Mom reports that within its assisted living network, over 96% of communities provide meals, nearly 98.6% offer incontinence care, and almost 90% offer medication management. These statistics are based on their proprietary network data for 2025, so while not a national census, they offer a realistic picture of what many communities deliver.

The Role of Occupational Therapy in Slowing Decline
Occupational therapy (OT) is one of the most effective — yet underutilized — resources for maintaining function at every stage of decline. An occupational therapist evaluates how a person performs ADLs and IADLs in their actual living environment and recommends compensations, modifications, and training to maximize independence.
For someone in the early IADL-loss stage, an OT might introduce a pill-sorting system, a simplified checkbook ledger, or a memory-aid app. For a person who has begun to struggle with bathing, an OT can recommend a shower chair, grab bar placement, and a no-rinse shampoo routine. Even at advanced stages, OT can help caregivers learn safe transfer techniques or positioning to prevent pressure injuries.
Several assessment tools reviewed in the 2020 systematic review — including the Katz Index, Lawton Scale, Barthel Index, and Functional Independence Measure (FIM) — are commonly used by OTs to establish a baseline and track change over time. This objective measurement helps families see where the person is improving (even if slowly) and where additional support is needed.
When ADL Assessment Triggers Insurance Benefits
ADL assessment is not just a clinical tool — it is the gatekeeper for many long-term care benefits. Most long-term care insurance policies and the VA Aid and Attendance pension require the inability to perform at least two ADLs without hands-on assistance before benefits begin.
The six ADLs typically used by insurers are bathing, eating, dressing, transferring, toileting, and continence (the same six in the Katz Index). According to ERISA Attorneys, even needing prompting or direction — such as a caregiver saying "it's time to bathe" and guiding hands-on — can qualify as an inability to perform an ADL. The key is that the person cannot do the task independently; the level of assistance needed determines eligibility.
For long-term care insurance, the standard trigger is needing hands-on assistance with at least two ADLs. For the VA Aid and Attendance benefit, the same two-ADL requirement applies, with the addition that the veteran must also need supervision or protection from everyday hazards. Because the clock starts ticking once ADLs are documented, families should not wait until a crisis to have the assessment done.
- Document which specific ADLs are impaired and the level of assistance (reminding, cueing, physical help).
- Obtain a signed statement from the primary care provider or specialist.
- Keep a log of care needs over one to two weeks to substantiate the claim.
- Submit the claim early; benefits often have a 90-day elimination period before payouts begin.
Understanding this administrative side of functional decline — even while it feels distant from daily care — can mean the difference between affording a home health aide and exhausting savings within months. Better Health While Aging emphasizes that ADL/IADL assessments are often required to trigger long-term care insurance benefits, making it essential for caregivers to understand how they work.
Key Takeaways for Family Caregivers
Functional decline in dementia, frailty, and other age-related conditions follows a pattern that is both predictable and actionable. By understanding that IADLs erode first and basic ADLs follow, caregivers can spot early signs, introduce support gradually, and avoid the scramble that comes with unexpected crises.
- Watch for IADL changes — unpaid bills, missed pills, uneaten groceries, abandoned hobbies. These are often the first clues that something is wrong.
- Get a baseline assessment — ask the primary care provider for an ADL/IADL evaluation using the Katz Index or Lawton Scale. A numerical score makes it easier to track change over time.
- Consult an occupational therapist early — OT can provide compensatory strategies and home modifications that stretch the window of independence.
- Plan support progressively — introduce meal services, medication management, and part-time home care during the IADL-loss stage; scale to personal care and residential options as ADL needs emerge.
- Document ADL needs for insurance — a physician’s statement specifying two or more ADLs requiring assistance can unlock long-term care insurance or VA benefits.
- Expect different trajectories — Alzheimer’s tends to take the IADL-first path; stroke, hip fracture, or vascular dementia may cause sudden, stepwise declines that require more immediate adjustments.
No two caregiving journeys look exactly alike, but the IADL-to-ADL framework gives you a roadmap. When you know what to look for and what comes next, you can make decisions from a place of understanding rather than panic — and that makes all the difference for both you and the person you care for.
Last reviewed: June 11, 2026
Browse more in the Glossary.