
Glossary entry
PERS (Personal Emergency Response System): Definition, How It Works, and Coverage

Why the Name Varies: PERS, Medical Alert System, MERS, and Life Alert
If you have seen the acronym PERS in a hospital discharge summary, a social worker's assessment, or a Medicaid waiver document, you have already encountered the formal clinical and regulatory name for what most families call a medical alert system or, informally, a life alert.
The terminology varies by context, not by device. CMS, state Medicaid agencies, occupational therapists, and policy documents use PERS because it is precise and vendor-neutral. Families and consumer media most often say medical alert system or medical emergency response system (MERS). "Life alert" (lowercase) is a consumer colloquialism that derives from a brand name — it is widely understood but is not a generic industry term.
All of these names refer to the same category of device and service. When a clinician writes "PERS" in a care plan, they mean the same thing a family member means when they say "we should look into a medical alert button for Mom."
How a PERS Works: Three Components and the Activation Sequence
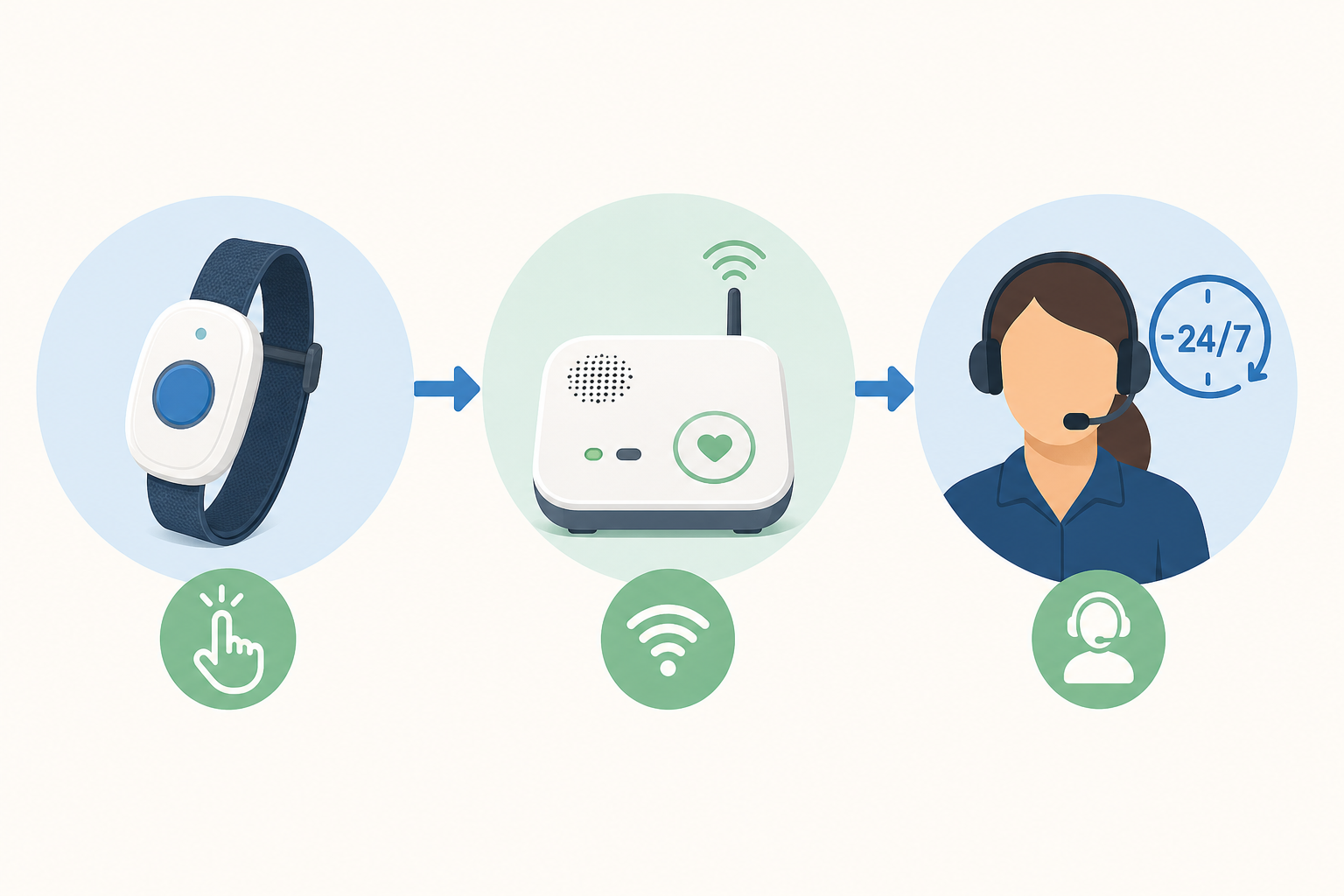
A standard PERS has three core components working together. Understanding each one helps caregivers evaluate whether a given system fits the user's living situation and communication needs.
- Wearable radio transmitter — a small device worn as a pendant around the neck, a wristband, or a clip-on. The user presses its button to trigger an alert. It must be worn consistently to be effective — including in the bathroom, where many falls occur. Waterproofing is a standard requirement in regulatory specifications.
- Base console — a home unit connected to a telephone landline or cellular network. It receives the signal from the wearable transmitter and places the call to the monitoring center. It includes a speaker and microphone for two-way voice communication, allowing the user to speak with an operator from anywhere within range.
- 24/7 emergency response monitoring center — a staffed call center that receives the alert, assesses the situation through two-way voice communication, and takes action: notifying designated emergency contacts, dispatching emergency services, or both. The operator remains on the line until help arrives.
The activation sequence from button press to operator response typically takes under 60 seconds: the wearable transmits a signal to the base console, the console automatically dials the monitoring center, and a live operator connects via the console's speaker and microphone to assess what kind of help is needed.
Five Types of PERS: A Capability Spectrum
PERS systems range from basic home-only pendants to GPS-enabled mobile devices and passive detection systems that require no button press at all. The right type depends on the user's living situation, mobility, and cognitive ability.
| Type | How It Works | Best Suited For | Key Limitation |
|---|---|---|---|
| Home landline | Transmitter communicates with a base console connected to an active telephone landline | Users with a working landline who stay primarily at home | Requires a landline; range limited to the home and immediate surroundings |
| Home cellular | Same in-home function as landline type, but uses a cellular network instead of a phone line | Users without a landline who stay primarily at home | Requires cellular signal in the home; same range limitation as landline type |
| Mobile / GPS | Works anywhere with cellular coverage; includes GPS location tracking so operators can identify the user's location | Active seniors who spend time outside the home; users who drive or travel | Ongoing cellular service required; battery must be charged regularly |
| Automatic / passive fall detection | Detects a fall without requiring the user to press a button, using wearable accelerometers or ambient sensors (radar, infrared, or camera-based) | Users with cognitive impairment, limited hand strength, or a history of falls who may not be able to press a button | Detection accuracy varies; some systems have false-positive rates; ambient sensors require installation |
| App-based | Smartphone application with one-touch SOS calling, GPS location sharing, and some fall detection capability | Smartphone-comfortable users who want a lower-cost option integrated into an existing device | Depends on the user having and carrying a charged smartphone; some configurations lack a dedicated 24/7 monitoring center |
Why Rapid Response Matters: The 'Long Lie' and Rhabdomyolysis
The clinical urgency behind PERS comes from what happens when an older adult cannot get up after a fall and remains on the floor — a situation researchers call the "long lie." Lying on a hard floor for an hour or more can cause rhabdomyolysis, a condition in which muscle tissue breaks down and releases its contents into the bloodstream. Rhabdomyolysis can lead to kidney failure and, in older adults, is life-threatening.
"The last thing you want is for an older person to be on the floor for an extended period of time. Not only is it emotionally traumatic, but they could develop rhabdomyolysis, a life-threatening condition that occurs when muscle tissues break down and release their contents into the bloodstream. It can happen when lying on the floor for as little as an hour." — Dr. Warren Wong, geriatrician, as quoted by AARP
Beyond rhabdomyolysis, a long lie can cause dehydration, pressure sores, and internal bleeding. A systematic review published in the Journal of Geriatric Physical Therapy (Chaudhuri, Thompson & Demiris, 2014) found that a long lie occurred in approximately 30% of fallers in a prospective cohort study, and that half of those who experienced a long lie died within six months of the fall. These figures are drawn from studies conducted between 2008 and 2014; no more recent peer-reviewed equivalent was identified at the time this entry was reviewed.
Who Typically Uses PERS and When It Is Recommended
PERS is most commonly recommended for older adults whose living situation or health history creates a meaningful risk of an unwitnessed emergency. Formal recommendations come from healthcare providers — occupational therapists, physical therapists, physicians, and social workers — based on individual assessment.
Populations for whom PERS is frequently recommended include:
- Older adults who live alone or who are alone for significant portions of the day
- Individuals with a documented fall history or a high clinical fall risk
- People managing chronic conditions that can cause sudden incapacitation — including heart disease, epilepsy, and diabetes
- Patients recovering from surgery or a hospitalization who are at elevated fall risk during the recovery period
- Individuals with cognitive impairment who may not be able to recognize or respond to an emergency without prompting
- People with physical disabilities that limit their ability to reach a telephone or call for help independently
Common recommendation triggers include hospital discharge (particularly after a fall-related admission), a social worker's home safety assessment that identifies extended caregiver absence, and documented fall history that has not yet resulted in serious injury.
Medicare and Medicaid Coverage Overview
Coverage options do exist through other programs, and the landscape varies significantly by plan and by state.
| Coverage Source | Coverage Status | Key Details |
|---|---|---|
| Original Medicare (Parts A & B) | Not covered | PERS is not classified as DME under CMS rules; no reimbursement available through standard Medicare |
| Medicare Advantage (Part C) | Varies by plan | Some plans offer partial or full PERS coverage as a supplemental benefit; eligibility and reimbursement amounts differ by plan and change annually — check your specific plan's Evidence of Coverage document |
| Medicaid HCBS Waivers | Available in 48 states and D.C. | The most common funding source; typically reimburses $25–$75/month for ongoing monitoring plus a one-time $40–$200 startup/installation reimbursement; waiver details vary by state |
| Consumer-Directed Medicaid Services | State-dependent | Allows beneficiaries to select and direct their own PERS service within Medicaid-approved parameters |
| State PCA Programs | State-dependent | Some state Personal Care Attendant programs include PERS as a covered support service |
| Money Follows the Person | State-dependent | Available for individuals transitioning from nursing facility care back to community living; PERS may be included as a community support service |
For Medicaid, the HCBS waiver pathway is the most broadly available. According to PayingForSeniorCare.com's Medicaid PERS coverage resource, 48 states and Washington D.C. offer some form of financial assistance for PERS through Medicaid. Dollar ranges and eligibility criteria differ significantly from state to state, and state waiver program details change on a regular basis.
Related Terms in This Glossary
Clinical and policy documents that use the term PERS often reference related concepts. The following terms frequently appear in the same discharge summaries, care plans, and Medicaid waiver documents:
- Fall detection — the capability (built into some PERS devices) to automatically detect a fall using accelerometers or ambient sensors, without requiring the user to press a button. Distinct from a standard PERS, which requires manual activation.
- HCBS waiver — Home and Community Based Services waiver; the Medicaid program structure through which most states fund PERS for eligible older adults and individuals with disabilities.
- Aging in place — the goal of remaining safely at home as health and mobility change; PERS is one of the tools that supports aging in place by providing a safety net for unwitnessed emergencies.
- ADL (Activities of Daily Living) — the basic self-care tasks (bathing, dressing, eating, toileting, transferring, continence) used to assess functional independence. ADL limitations are often part of the clinical picture that triggers a PERS recommendation.
- DME (Durable Medical Equipment) — the Medicare category covering reusable medical devices prescribed for home use (e.g., wheelchairs, walkers, hospital beds). PERS is not classified as DME under current Medicare rules, which is why Original Medicare does not cover it.
Browse more in the Glossary.