
Wandering in Dementia: A Room-by-Room Home Safety Audit and Monitoring Technology Guide
For caregivers who have already recognized wandering as an active or emerging risk, this guide provides a systematic room-by-room home safety audit framework and a product-neutral technology evaluation rubric to help build a layered, stage-aware wandering prevention system before a crisis occurs.
If you've already recognized that your family member is at risk for wandering, you're past the point of needing a general explanation. What you need now is a systematic way to assess your home and a clear framework for evaluating the monitoring technology that could help keep them safe. This guide is built for that moment.
Why Physical Modifications and Monitoring Technology Work Together
No single intervention reliably prevents elopement. Door locks can be defeated. Visual deterrents lose effectiveness as dementia progresses. Monitoring devices can go uncharged or be removed. The caregivers who manage wandering risk most successfully treat it as a layered problem — one that requires both physical changes to the environment and a technology system that alerts when those physical barriers are tested.
The stakes are high. Of individuals who are not found within the first 24 hours after wandering, 50% end up either severely injured or dead. Nighttime wandering is particularly dangerous — the person is more likely to be disoriented, there are fewer people outside who might notice, and a sleeping caregiver may not realize anything has happened until morning.
Physical modifications reduce the likelihood of exit. Monitoring technology reduces the time between an exit attempt and a caregiver response. Together, they provide a protection system that neither can offer alone.

How to Conduct a Wandering-Risk Home Audit
A wandering-risk audit is a systematic walk through your home with one question in mind: where could someone exit, and what would slow them down or alert you if they tried? You don't need a professional safety inspector to do this. You need a methodical approach and time to look at your home the way someone with dementia might navigate it.
Start by identifying every potential exit point — not just the front door. Many caregivers overlook secondary exits that become the path of least resistance once the primary door is secured.
- Front door and any secondary entry doors
- Back door and side doors
- Garage door — both the pedestrian door into the garage and the main garage door
- Basement door, especially if it leads outside
- Sliding glass doors to patios or decks
- Low windows that could be opened and climbed through
- Any gate or fence opening that leads to the street
Next, walk the interior paths that lead to those exits. Look for navigation hazards that could increase confusion or fall risk during a nighttime attempt: poor lighting in hallways, abrupt transitions between floor surfaces, and room layouts that don't clearly signal which way leads outside versus which way leads to a bedroom or bathroom.
Finally, step outside and assess the perimeter. Is there a fence? Does it have a gate, and is the gate latch operable by someone with moderate dementia? Are there areas where someone could exit the yard without going through a gate?
Room-by-Room Modification Guide
Once you've identified your exit points and navigation hazards, the following room-by-room modifications address the most common pathways. Prioritize the locations your audit identified as highest risk.
Entryways and Exterior Doors
Exterior doors are the primary target for modification. The goal is to make exit attempts less automatic — to introduce enough friction or visual confusion that the person pauses or abandons the attempt.
- Install a deadbolt above or below eye level. Dementia-related perceptual changes reduce awareness of unusual lock placement. A deadbolt positioned near the top of the door frame or near the floor is often overlooked by someone who has learned to reach for a handle at standard height.
- Use child-proof doorknob covers. These add a manipulation step that can interrupt the automatic sequence of reaching for and turning a handle.
- Apply visual deterrents at the door. A STOP sign or DO NOT ENTER sign near the door may be effective in early-to-moderate stages. A black floor mat or a two-foot black threshold area in front of the door may appear as an impassable barrier to someone with dementia-related depth perception changes.
- Camouflage the door. Painting the door the same color as the surrounding wall, covering it with a removable curtain, or hanging artwork on it can reduce its visual salience as an exit. Match the door handle color to the door color as well.
- Remove exit-cue items from entryways. Coats, hats, handbags, and car keys stored near the door can trigger the cognitive association of leaving. Moving these items out of sight reduces that prompt.
Bedroom and Nighttime Exits
Nighttime wandering typically begins with getting out of bed. The window between rising and reaching an exterior door can be very short, which makes early detection in the bedroom critical.
- Install nightlights throughout the path from the bedroom to any exit, including in the hallway and bathroom. Disorientation increases significantly in low light.
- Place a bed sensor (pressure pad or wearable button) to alert you when the person gets up. This is covered in more detail in the monitoring technology section below.
- Consider the bedroom door itself — a simple door alarm that chimes when opened gives you an additional alert layer between the bed and the exterior.
Bathroom
The bathroom is less often an exit point but is a common destination for nighttime disorientation. Clear labeling on the bathroom door (a simple sign at eye level) and a nightlight inside the bathroom reduce the likelihood that someone waking up confused will wander toward an exterior door while searching for the toilet.
Garage and Basement
Garages and basements are high-risk exit points that are often overlooked because they don't feel like "front doors." They also contain tools, chemicals, and equipment that create secondary hazards if someone enters these areas unsupervised.
- Install a motion-sensor light or alarm on the garage door — both the main door and the pedestrian door that connects the garage to the house.
- Add a keyed lock or high-mounted latch to the door between the house and the garage.
- Treat the basement door the same way — a latch above eye level and a door alarm are both appropriate here.
Outdoor Yard and Perimeter
For people who retain the ability to operate door hardware, a secured outdoor perimeter is the most reliable exit prevention available. A fenced yard with a locked gate allows supervised outdoor time while containing the person within a safe boundary.
A secure outdoor space can also reduce the urge to seek exit by providing a change of scenery and physical activity within a safe boundary. This is one of the few modifications that serves both prevention and quality of life simultaneously.
- Install a fence that cannot be easily climbed or pushed through, with a gate that requires a key or a latch mechanism the person cannot operate.
- Use safety gates or brightly colored netting to block access to stairs or areas with outdoor access.
- Check for gaps in hedges, low fence sections, or unlocked side gates that could serve as secondary exit points.
| Location | Primary Modification | Secondary Modification | Stage Effectiveness |
|---|---|---|---|
| Exterior doors | Deadbolt above/below eye level | Door camouflage or curtain; remove exit cues | Early–moderate; reassess at advanced stage |
| Bedroom | Bed sensor alert | Nightlights on exit path; bedroom door alarm | All stages |
| Hallways | Nightlights along baseboards | Path lighting to bathroom | All stages |
| Garage / basement | Keyed lock or high-mounted latch | Motion-sensor alarm on door | All stages |
| Outdoor perimeter | Locked fence and gate | Safe outdoor zone to reduce exit urge | Most effective when person can still operate doors |
Monitoring Technology Categories: What Each Does and When to Use It
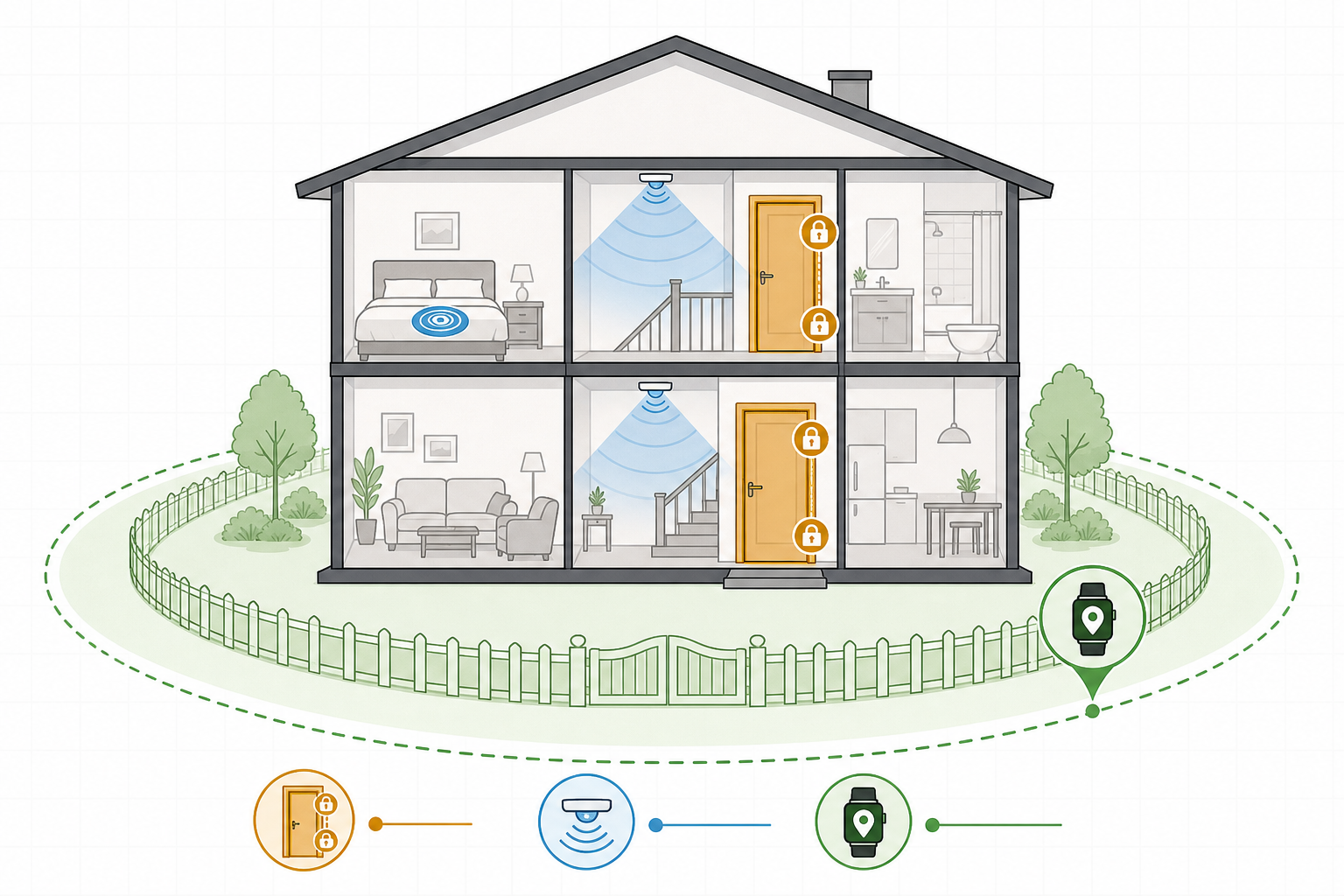
Monitoring technology for wandering falls into five categories. Each serves a different function, works best in different household situations, and carries distinct trade-offs. Understanding what each category does — and what it cannot do — is the foundation for building a system that works for your specific situation.
Door and Window Contact Sensors
Contact sensors are placed on door or window frames and trigger an alert when the door or window opens. They are among the simplest and lowest-cost options available. Basic models require no Wi-Fi and can alert via a standalone chime or pager. More connected models send smartphone notifications.
Their limitation is that they only detect an exit attempt after the door is already open. They do not prevent the attempt — they alert you to it. Response time depends entirely on how quickly the caregiver receives and acts on the alert.
Motion-Activated Alert Systems
Motion sensors detect movement within a defined area — typically a hallway, doorway, or room — and send an alert when triggered. Positioned between the bedroom and an exterior door, they can give caregivers an earlier warning than a door contact sensor alone, because they detect movement before the person reaches the door.
The trade-off is false alarms. A hallway motion sensor will trigger on any movement — a pet, a family member getting water at night, or the monitored person using the bathroom. Caregivers in households with multiple occupants often find motion sensors most useful when positioned specifically on exit paths rather than general living areas.
Bed and Chair Sensors
Bed and chair sensors detect when a person gets up from a sleeping or resting position. Two main designs exist: pressure pads placed under the mattress or cushion, and wearable button sensors clipped to clothing or bedding. Both trigger an alert when the person rises.
These are particularly valuable for nighttime wandering prevention because they give caregivers the earliest possible alert — at the moment of rising, before any movement toward a door. Wireless models with long battery life reduce the maintenance burden, which matters in a caregiving household where missed charging is a real risk.
GPS Wearables and Trackers
GPS trackers do not prevent wandering. What they do is dramatically reduce response time after elopement occurs. When someone leaves a safe area, a GPS tracker with geofencing capability sends an immediate alert and allows caregivers to see the person's location in real time.
Form factors include watch-style wearables, pendants, belt clips, shoe insoles, and portable trackers that can be placed in a bag or pocket. Each form factor involves a different compliance challenge — the person must be willing and able to wear or carry the device consistently.
Camera Monitoring with Two-Way Audio
Camera systems allow caregivers to visually check on a person remotely — particularly useful for long-distance caregivers or for caregivers who are in another part of the home. Models with two-way audio allow the caregiver to speak through the camera, which can redirect a person who is moving toward an exit.
Camera monitoring raises privacy and consent considerations that the other categories do not. These are addressed in the evaluation framework section below.
| Category | Primary Function | Key Limitation | Best Household Fit |
|---|---|---|---|
| Door / window contact sensors | Alerts when door or window opens | Detects exit after door is already open | Simple setups; single-caregiver households; no Wi-Fi required for basic models |
| Motion-activated alerts | Detects movement toward exits before door is reached | False alarms from other household movement | Households where exit path can be clearly isolated |
| Bed / chair sensors | Alerts when person rises from sleep or rest | Requires reliable charging; wearable versions need compliance | Nighttime wandering risk; caregiver sleeping in adjacent room |
| GPS wearables / trackers | Locates person after elopement; geofencing alerts | Does not prevent exit; requires compliance and charging | Active wanderers; outdoor risk; caregiver not always on-site |
| Camera with two-way audio | Remote visual check-in; verbal redirection | Privacy considerations; requires Wi-Fi; does not physically prevent exit | Long-distance caregivers; large homes; supplemental layer |
How to Evaluate Monitoring Technology: A Product-Neutral Framework
Once you've identified which technology category fits your situation, the next step is comparing options within that category. The following evaluation dimensions apply across all five categories and give you a structured way to assess options without relying on brand marketing.
Reliability and False-Alarm Rate
A system that generates frequent false alarms will be ignored or disabled. Ask specifically about false-alarm rates in household settings with pets, multiple occupants, or HVAC airflow that can trigger motion sensors. For contact sensors, ask whether the sensor distinguishes between a door opening fully versus a brief partial opening.
Caregiver Alert Method
How the alert reaches you — and how quickly — determines whether the system is useful at 3 a.m. Key questions: Does the alert go to a dedicated pager, a smartphone app, or both? Can multiple caregivers receive alerts simultaneously? How long does the alert continue if not acknowledged? Pager-style alerts are often preferable to smartphone apps for overnight use because they don't require unlocking a phone.
Battery Life and Charging Burden
Missed charging is one of the most common failure points in dementia monitoring systems. A device that needs daily charging will eventually be found dead at the moment it's needed. For GPS trackers specifically, battery life varies significantly — basic models last one to three days, while more advanced models can last a week or more. Longer battery life is worth prioritizing even if it comes at a higher cost.
Compliance and Wearability
For wearable devices, the most sophisticated GPS tracker is useless if the person removes it. Ask whether the device is designed to be worn discreetly, whether it can be placed inside clothing or shoes rather than on the body, and whether there are options for people who actively resist wearing devices. Hidden trackers placed in shoe insoles or sewn into a jacket lining maintain monitoring without requiring active cooperation.
Indoor Location Accuracy
GPS alone performs poorly indoors — satellite signals are blocked by walls and roofs. Devices that combine GPS with Wi-Fi positioning and cellular triangulation provide significantly better indoor accuracy. If you need to locate someone inside a building or in a densely developed neighborhood, this distinction matters.
Privacy and Consent
Monitoring a cognitively impaired person raises genuine ethical questions about privacy and dignity. Camera systems in particular require careful thought about placement — a camera in a bedroom or bathroom is a significant privacy intrusion even when the person cannot fully consent. The general principle: use the least intrusive technology that provides the necessary level of safety. Discuss monitoring plans with the person's care team and, where the person retains capacity to participate, involve them in the conversation.
Total Cost Structure
Many monitoring systems involve both a one-time hardware cost and an ongoing monthly subscription for cellular connectivity, monitoring services, or cloud storage. A device with a low upfront price may carry a higher total cost over 12 to 24 months than a more expensive device with no subscription. Calculate the 24-month total cost when comparing options, not just the purchase price.
| Evaluation Dimension | What to Ask | Why It Matters |
|---|---|---|
| Reliability / false-alarm rate | How often does the system trigger without a real event? | Frequent false alarms lead to alert fatigue and system abandonment |
| Caregiver alert method | Pager, app, or both? How many caregivers can receive alerts? | Alert delivery at 3 a.m. determines whether the system is actually useful |
| Battery life | How many days between charges? What happens when battery is low? | Missed charging is a common failure point in dementia care households |
| Compliance / wearability | Can it be worn discreetly or hidden? What if the person removes it? | A device that is removed provides no protection |
| Indoor accuracy | Does it use GPS only, or GPS + Wi-Fi + cellular? | GPS alone is unreliable indoors and in dense neighborhoods |
| Privacy and consent | Where will it be placed? Has this been discussed with the care team? | Monitoring cognitively impaired individuals raises dignity considerations |
| Total cost structure | What is the 24-month total including hardware and subscription? | Low upfront cost can obscure a high ongoing subscription burden |
Building a Layered Safety System Across Disease Stages
The modifications and technology that work at one stage of dementia may be insufficient — or may need to change — at the next. Building a layered system means thinking about how physical modifications and monitoring technology work together, and planning for reassessment as the disease progresses.
A key principle from the Family Caregiver Alliance applies directly here: what works today may not work tomorrow. Visual deterrents that are effective in early-stage dementia lose their effect as the disease advances. Locks that were sufficient at moderate stages may need to be supplemented with alarms at advanced stages. The system you build now should be treated as a starting point, not a permanent solution.
| Disease Stage | Wandering Risk Profile | Physical Modifications Priority | Monitoring Technology Priority |
|---|---|---|---|
| Early stage | Emerging risk; occasional disorientation; may still respond to verbal redirection | Visual deterrents (STOP signs, black mats); remove exit cues; high/low deadbolts | Door contact sensors; basic motion alerts near exits |
| Moderate stage | Highest wandering risk period; visual deterrents losing effectiveness; may not respond to verbal cues | Physical locks prioritized over visual deterrents; perimeter fencing if outdoors accessible; bedroom door alarms | Bed sensors for nighttime; GPS tracker if outdoor access possible; door alarms on all exits |
| Advanced stage | Wandering less common due to reduced mobility, but still possible; physical barriers most important | Full lock coverage on all exits; remove or restrict access to garage and basement | Bed sensors remain valuable; GPS less critical if mobility is significantly reduced; camera monitoring for supervision |
Technology supplements physical modifications — it does not replace them. A GPS tracker tells you where someone is after they've left. A door alarm tells you a door has opened. Neither prevents the exit. Physical modifications — locks, visual deterrents, perimeter fencing — are the barriers. Technology is the alert system that gives you time to respond when those barriers are tested.
Emergency Preparedness: The Wandering Kit and 15-Minute Protocol
Even a well-designed safety system can be defeated. Assembling an emergency preparedness kit and practicing a response protocol before an incident occurs dramatically improves outcomes if one does happen. This preparation should happen now, not after a wandering event.
Assemble the Wandering Kit
- A recent, close-up photograph showing the person's face clearly. Update this every three to six months. This is what you will give to police if you call 911.
- A medical summary including the person's name, diagnosis, physical description, and any medical conditions that could affect how they respond to first responders.
- A list of likely destinations. People with dementia who wander often head toward places that were meaningful earlier in life — a former home, a previous workplace, a place of worship, a family member's house. Write these down with addresses.
- Contact information for neighbors, nearby family, and local law enforcement's non-emergency line.
The 15-Minute Search Protocol
- Search the home and immediate outdoor perimeter first — including any outbuildings, the garage, and the backyard. Many wandering incidents are resolved within the immediate property.
- If not found within 15 minutes, call 911 immediately. Do not wait longer. Provide the officer with your prepared photo and medical summary.
- Alert your neighbor network simultaneously. Neighbors who know the person and understand the situation can cover more ground quickly.
- Note the direction of travel if you have any information. People who wander tend to move in the direction of their dominant hand. If you know the person is right-handed and exited through the front door, they are more likely to have turned right.
- Check the list of likely destinations and dispatch a family member or trusted neighbor to each one while you coordinate with police.
MedicAlert + Alzheimer's Association Safe Return
Enrolling in the MedicAlert + Alzheimer's Association Safe Return program provides 24-hour nationwide emergency assistance. The program registers the person's information and provides an identification bracelet or necklace. If the person is found by someone who does not know them, a call to the program's number connects first responders or good samaritans to you. Enrollment should be completed before any wandering incident occurs.
When Home Modifications Are No Longer Enough
There is a point in some dementia trajectories where the home environment — even a well-modified one — cannot safely manage wandering risk. Recognizing that point is important. It is not a failure of caregiving; it is a recognition that the person's needs have exceeded what the home environment can provide.
Consider discussing the current safety plan with the person's care team if any of the following are occurring:
- Wandering incidents are becoming more frequent or are now occurring nightly despite modifications.
- The person is consistently removing monitoring devices or finding ways around physical modifications.
- A safety incident — an exit that was not detected, an injury during a wandering episode — has already occurred.
- The caregiver's sleep is so disrupted by nighttime monitoring that their own health and judgment are being affected.
- The modifications required to maintain safety are creating a living environment that significantly diminishes the person's quality of life.
A layered safety system — physical modifications combined with monitoring technology, reassessed at each stage transition — is the strongest approach available for managing wandering risk at home. Building that system before a crisis, and maintaining it as dementia progresses, is the most important step caregivers can take.
Related reading
Noticed something outdated or inaccurate on this page? Flag a correction. We review every report against CDC, NIA, and AARP HomeFit guidance before updating a page.
Part of the Fall Prevention section.