How to Match Your Caregiver Burnout Symptoms to the Right Respite Option
Reviewed: 2026-07-05
How to Match Your Caregiver Burnout Symptoms to the Right Respite Option
Learn how to identify which caregiver burnout symptom cluster you're experiencing—physical, emotional, behavioral, or cognitive—and find the specific type of respite care that matches your situation, whether in-home help, adult day care, or a multi-day residential break.
By Editorial Team
new caregiver
experienced caregiver
long-distance caregiving
spousal caregiver
working caregiver
daily routines
medication management
personal hygiene
care coordination
first steps
ADLs
IADLs
If the main thing you notice is your body shutting down, your emotions going flat or hot, your behavior shrinking, or your thinking becoming foggy, that pattern can point to a different kind of break. More than 60% of caregivers experience symptoms of burnout, according to Cleveland Clinic, so the fact that you are looking for language for this does not mean you are failing at care.[1]
The more useful question is not “Do I deserve a break?” It is “What kind of break matches the damage caregiving is doing right now?” A few hours away can help one caregiver. For another, it barely scratches the surface because the problem is not an afternoon errand; it is months of never being psychologically off duty.
Start With the Symptom That Is Running the House
Caregiver stress often shows up in overlapping ways. Mayo Clinic points caregivers to warning signs such as feeling overwhelmed, sleeping too much or too little, gaining or losing weight, becoming easily irritated or angry, losing interest in activities, and feeling tired often.[2] Caregiver Action also distinguishes ordinary burnout from compassion fatigue, where emotional exhaustion can make a loving person feel detached, numb, or unable to respond with the tenderness they expect from themselves.[3]
You may recognize more than one cluster. That is normal. For choosing respite, begin with the cluster that is creating the most risk: the symptom that is making you unsafe, unreliable, unreachable, or unable to recover between care tasks.
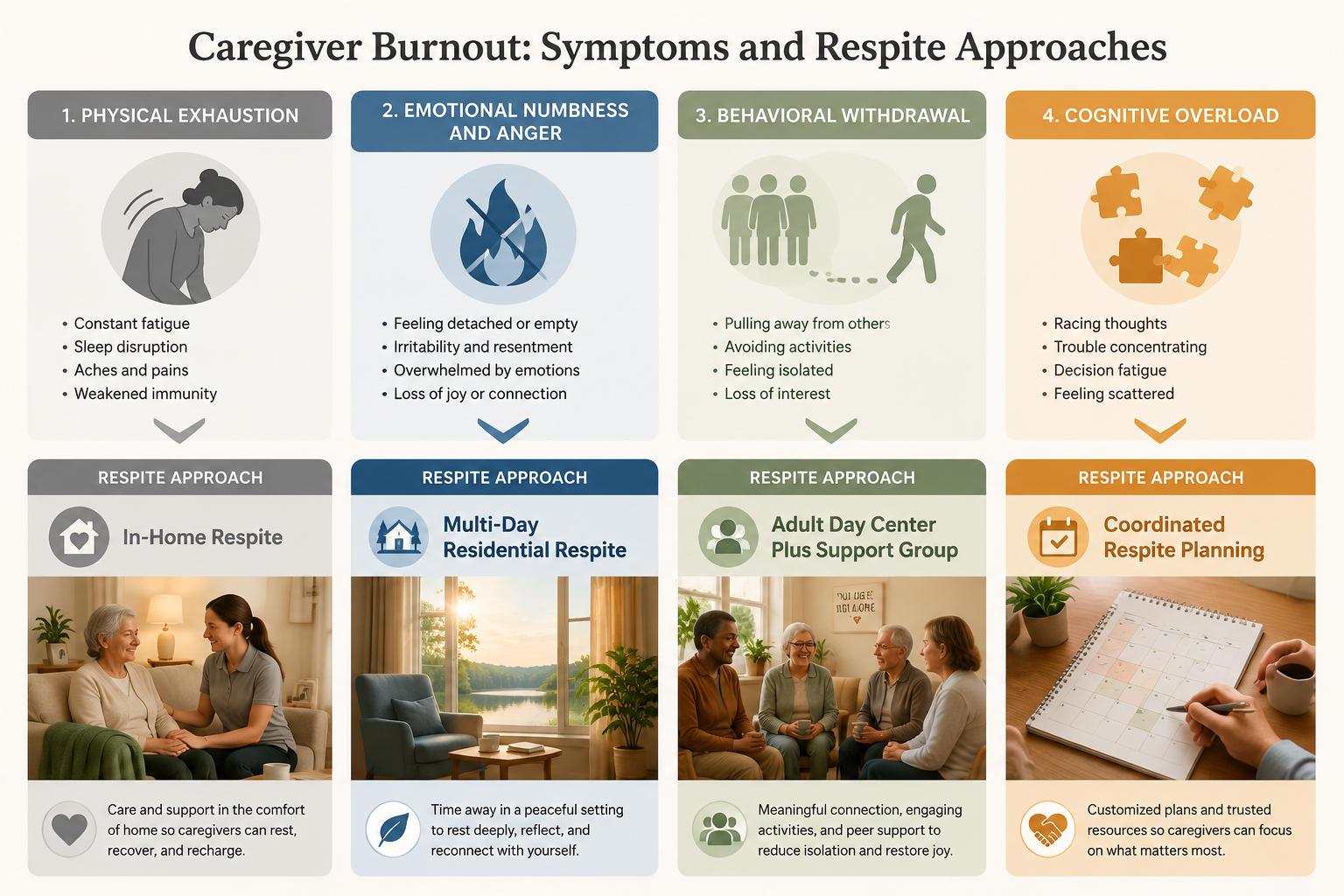
Dominant symptom cluster
What it may sound like in real life
Best first respite match
Why this match fits
Physical exhaustion
“I can’t sleep enough to feel human. My back hurts. I’m getting headaches. I dread the next transfer, shower, or night wake-up.”
In-home respite for several hours at a time, repeated if possible
It reduces the caregiver’s physical load without forcing the parent through a major setting change.
Emotional numbness, anger, or compassion fatigue
“I feel nothing when Mom calls again. Or I feel rage, then shame. A few hours off does not reset me.”
Multi-day residential respite or short-term stay when feasible
It creates a protected stretch of time long enough for emotional recovery, sleep, and distance from constant vigilance.
Behavioral withdrawal
“I cancel plans, stop answering texts, avoid siblings, and only leave the house for care tasks.”
Adult day care plus a caregiver support group
The parent gets structured daytime care while the caregiver’s isolation is treated as part of the problem.
Cognitive overload
“I forget appointments, miss forms, reread messages, and lie awake planning the next problem.”
Respite with coordination help or a longer planning window
The break has to remove some management work, not just free a few empty hours.
ARCH National Respite Network describes respite across several settings, including in-home care, adult day services, and short-term residential options.[4] Those are not interchangeable menu items when you are exhausted. Setting, duration, and transition burden matter because the wrong kind of respite can add another job to your list.
When Your Body Is the Alarm: Choose the Lowest-Transition Break
Physical burnout is often the easiest to dismiss because it can look like ordinary tiredness. The difference is that ordinary tiredness improves after rest. Caregiving exhaustion can keep accumulating because the night shift, medication schedule, fall risk, meals, laundry, and appointments do not pause just because your body asked nicely.
If your main symptoms are headaches, muscle pain, sleep disruption, stomach trouble, frequent illness, or the sensation that you are moving through the day with a drained battery, in-home respite is often the cleanest first step. Someone comes into the existing care environment, and your parent does not have to adapt to a van ride, a new room, new staff, or a full-day program before you can lie down.
This is where a smaller break can be more practical than a dramatic one. If your parent becomes frightened or disoriented in unfamiliar places, arranging an outside stay may require so much preparation that it consumes the energy you were trying to regain. In-home respite can cover the shower routine, a meal block, a medical appointment window, or the hours when you usually cannot let your attention drop.
The goal is not to “do something nice for yourself” in the abstract. The goal is to stop a specific bodily demand. Sleep in another room. Take a walk without watching the clock. Go to your own appointment. Sit in the car and answer no one. For physical exhaustion, the right respite is the one that removes hands-on duty quickly enough that your nervous system believes the break is real.
When You Feel Numb, Furious, or Unlike Yourself
Emotional burnout is the cluster people are most likely to hide. It can sound like, “I’m fine,” followed by a story about snapping at a parent, crying in the grocery store, resenting siblings, or feeling nothing when the person they love needs help again. The shame can be heavier than the symptom.
A few scattered hours may not be enough for this cluster because the problem is not only task fatigue. It is the constant emotional exposure: listening for the call, bracing for the next need, absorbing fear or confusion, and then judging yourself for not responding with endless patience. When compassion fatigue enters the room, distance is not abandonment; it is the condition that may allow compassion to come back.
This is where multi-day residential respite or a short-term care stay may be worth considering. In residential respite, the care recipient stays temporarily in a facility or care setting while the caregiver has a longer protected interval. ARCH includes residential respite among recognized respite models, and caregiver-facing guidance from Caregiver Action also treats respite as something that can be arranged in different settings depending on the family’s needs.[4][6]
The practical advantage is continuity. One afternoon off can disappear into grocery shopping, insurance calls, and guilt. Two or more nights can create a different kind of silence: no listening for footsteps, no medication alarm, no decision about whether to intervene. If you have been angry enough to scare yourself, numb enough to feel detached from your parent’s distress, or tearful every time you sit alone, a deeper break is not excessive.
The hard part is that this option can bring the most resistance. Your parent may say they do not want strangers. A sibling may decide the timing is inconvenient. You may feel as if you are proving some private accusation against yourself. Those reactions matter, but they should not automatically outrank the risk of a caregiver who is past the point of safe emotional recovery. If the conversation itself feels impossible, it may help to prepare it as a care-safety discussion rather than a request for permission; our guide to having hard conversations with aging parents goes deeper into that step.
For families considering a short-term facility stay after a hospitalization, fall, sudden decline, or caregiver crisis, the decision can overlap with broader short-term care planning. That is a different level of urgency than booking an afternoon helper, and it deserves a more careful look at safety, staffing, medication management, and discharge planning. Our short-term care decision guide can help if the respite need is tangled with a crisis placement.
When Your World Has Shrunk to the Care Routine
Behavioral burnout shows up less as one dramatic feeling and more as a narrowing life. You stop calling friends because there is too much to explain. You avoid family messages because they create work. You quit the exercise class, the book group, church coffee hour, Saturday errands with your spouse, anything that requires timing and coverage.
For this cluster, adult day care can do more than provide supervision. A good adult day center gives the care recipient somewhere to be: meals, activities, social contact, routine, and trained eyes during the day. That matters because the caregiver’s break is easier to protect when it is attached to a recurring program rather than renegotiated one favor at a time. If you need a fuller explanation of how this setting works, see our guide to adult day care for caregiver respite.
The caregiver side needs attention too. If your behavior has become isolated, respite should not only remove your parent from the house for a few hours. It should also reconnect you with people who understand the strain without making you perform gratitude or defend your choices. A caregiver support group can be especially useful here because it gives the break a destination that is not another errand.
This match is not perfect for every parent. Some people refuse group settings. Some programs are better equipped for memory loss, mobility limitations, or medical complexity than others. But when the caregiver’s life has narrowed to a hallway between the bedroom, kitchen, pharmacy, and phone, a recurring daytime structure can create the first reliable opening.
When Your Brain Is Carrying Too Many Tabs
Cognitive overload is the cluster that can make a competent person feel unreliable. You forget the appointment you scheduled. You miss a refill. You reread the same portal message three times. You wake at 3 a.m. trying to remember whether the insurance card, advance directive, walker order, lab result, and sibling update are all handled.
If this is your dominant pattern, “take a few hours off” may be too small because the work follows you. You can be sitting at lunch with a friend and still mentally triaging the next week of care. The respite match here is help that includes coordination relief: a service that helps arrange care, an agency that can fill predictable blocks, a day program with a reliable calendar, or a family plan where someone else owns a defined administrative lane.
The key is to remove decisions, not merely minutes. A sibling who says “tell me what to do” may mean well, but that still leaves the burned-out caregiver as dispatcher. A better offer is specific: “I will call three agencies and ask about Tuesday and Thursday coverage,” or “I will take over the medication refill calendar for the next month.” Our guide to coordinating a parent’s care without burning out focuses on that management load.
This is also the cluster where a longer planning window matters. If you are already missing details, do not make the first respite attempt depend on a complicated one-day scramble. Pick one repeatable block, one service category, and one person or office to call. The less heroic the plan, the more likely it is to happen.
Duration Matters More Than the Label
Once you know the symptom cluster, adjust the duration. The same respite setting can either help or disappoint depending on how much recovery time it actually creates.
A few hours may fit physical exhaustion when you need sleep, a medical appointment, errands, or a pause from hands-on tasks.
A recurring weekly block may fit behavioral withdrawal because it rebuilds rhythm and gives the caregiver a protected social or support space.
A full day or several days may fit cognitive overload when planning, calls, and paperwork need to be moved off your plate in an organized way.
A multi-day residential stay may fit emotional numbness, anger, or compassion fatigue because recovery may require uninterrupted nights and real psychological distance.
There is no moral ranking here. In-home respite is not “less serious,” and residential respite is not “giving up.” The right duration is the one that matches the symptom you are trying to interrupt.
Cost and Availability Can Change the Answer
The cleanest clinical match still has to survive the real world: money, openings, transportation, eligibility rules, and whether anyone in your area provides the service you need. National median cost estimates for 2026 put in-home respite around $33 per hour, adult day care around $106 to $115 per day, and short-term assisted living respite around $206 per day, with significant state and regional variation.[5]
Those numbers are not quotes for your family. They are starting points for deciding what to ask next. A rural area with few providers, a high-cost metro area, dementia-related supervision needs, weekend coverage, or personal care requirements can change the price and availability quickly.
Possible funding doors may include Medicaid waiver programs, veterans benefits, state respite vouchers, dementia-related caregiver support programs, nonprofit grants, or local aging-service funds. ARCH’s respite payment guidance points caregivers toward federal, state, and community funding routes, but these programs vary by location and eligibility.[4] For dementia caregivers, some families may also want to check whether a local provider participates in Medicare’s GUIDE model; our GUIDE model explainer explains what to verify before counting on it.
If the financial side is the part that keeps stopping you, start with your local Area Agency on Aging, Aging and Disability Resource Center, or state respite coalition rather than a broad internet search. Ask three concrete questions: what respite programs serve my ZIP code, what eligibility rules apply, and whether there is a voucher, sliding scale, or caregiver support fund. For a broader way to map possible help, see The Hidden $7,200 Gap.
Guilt Is a Barrier, but It Is Not a Care Plan
Caregiver guilt can make even a well-matched respite plan feel suspect. NCOA describes respite as temporary relief for caregivers and notes that it can be provided in different ways, including at home, in adult day programs, or in residential settings.[8] Still, knowing respite exists does not erase the feeling that a “good” daughter, spouse, or son should somehow absorb the whole load.
The guilt deserves compassion, not the steering wheel. If the parent is safe, fed, supervised, and treated with dignity, the caregiver’s recovery is part of the care system. It is not a side benefit. It is what keeps the system from depending on one exhausted person’s ability to keep overriding their own limits.
A useful first script is plain: “I am arranging coverage because I need to be able to keep doing this safely.” That sentence does not invite a courtroom debate about whether you are tired enough. If guilt is the main thing blocking you, our caregiver self-care checklist that gives you permission to care for yourself may be a better next read than another list of services.
A Quick Way to Choose Your First Call
Kingston Healthcare describes a four-stage caregiver burnout progression from warning signs to control, survival, and burnout; that kind of model can be useful for self-recognition, but it should not be treated as a formal diagnosis.[7] For today’s decision, you do not need to stage yourself perfectly. You need one workable next move.
Name the dominant cluster: physical, emotional, behavioral, or cognitive.
Match the setting: in-home respite, residential respite, adult day care with support, or coordination-focused respite.
Choose the minimum useful duration: hours, a recurring day block, a full day, or several days.
Call one local source: Area Agency on Aging, Aging and Disability Resource Center, state respite coalition, adult day center, home care agency, or short-term care provider.
Ask what is available, what it costs, what funding exists, and how soon coverage could realistically start.
If you still cannot tell which category fits, look at what would make the next 72 hours safer. If sleep would change everything, start with in-home help. If you are afraid of your own anger or numbness, ask about a longer stay. If isolation is closing in, look at adult day care and a support group. If the calendar and calls are breaking you, ask for coordination help before you ask for another vague break.

Comments
Join the discussion with an anonymous comment.