
Room checklist
Bedroom Modifications for Seniors Aging at Home: A Safety and Accessibility Guide
The bedroom is one of the most overlooked fall risk zones in the home — especially during nighttime bathroom trips. This guide walks family caregivers and older adults through a priority-tiered framework of bedroom modifications, from immediate low-cost actions to structural changes, with 2026 cost ranges, funding pathways, and guidance on when to bring in a professional.

Why the Bedroom Is a High-Risk Fall Zone
Most fall prevention conversations start with the bathroom. The bedroom deserves equal attention — and for a specific, time-bounded reason: the trip from bed to bathroom between midnight and 6 AM is among the most dangerous moments in a senior's day.
The scale of the problem is significant. Over 14 million adults ages 65 and older report falling every year — roughly one in four — and the age-adjusted fall death rate rose 21% between 2018 and 2024, reaching 78.4 deaths per 100,000 in 2024, according to the CDC National Vital Statistics System. Falls are now the leading cause of both fatal and nonfatal injuries among older adults.
Research published through a 2025 systematic review of home modification studies (Cha, Healthcare 2025) found that bathrooms and bedrooms together account for the majority of in-home falls among older adults. The bedroom's particular danger is situational: a person waking at 2 AM is disoriented, not fully alert, likely moving without glasses or hearing aids, navigating in low or absent light, and transitioning from a lying position — all of which compound the risk of losing balance.
The good news is that bedrooms are highly modifiable. Many of the highest-impact changes cost under $30 and can be done tonight. This guide organizes those changes by urgency and cost, so you can act immediately on what matters most and plan methodically for what comes next.
Five Bedroom Hazard Categories to Know
Understanding why bedroom falls happen makes the modifications more intuitive — and helps you prioritize. These five hazard categories cover the root causes, not just the symptoms.
- Bed transfer mechanics. Getting in and out of bed requires a controlled transition from lying to sitting to standing. When a bed is too high or too low, this transfer becomes unstable. A mattress that is too soft creates an uneven base; a frame without a stable edge makes it harder to push up. The transfer is a moment of peak instability, and it happens multiple times each night.
- Nighttime bathroom trips in the dark. This is the highest-risk scenario for bedroom falls. The person is partially asleep, blood pressure may drop on standing (orthostatic hypotension), and the room is dark. Without a lit path from bed to door, the risk of tripping on furniture, a rug, or a cord is substantially elevated.
- Inadequate lighting. Overhead ceiling lights are rarely on during nighttime trips, and reaching for a lamp switch requires moving in the dark first. Older adults also experience reduced night vision and slower pupil adaptation to light changes, meaning the transition from complete darkness to a bright overhead light creates a temporary visual gap.
- Improper bed height. A bed that is too high forces the person to lower themselves onto it from a height, increasing the risk of a backward fall. A bed that is too low makes standing up difficult and requires more hip and knee strength than many older adults have. Both extremes create unnecessary fall risk at a moment that happens every morning.
- Clutter, unsecured rugs, and loose cords. Throw rugs are among the most common household trip hazards. Their edges curl, they slide on smooth floors, and they catch shuffling feet or walker legs. Extension cords and phone charger cables running across the floor create the same risk. Clutter — laundry, shoes, reading materials — narrows pathways and introduces unpredictable obstacles in the dark.
Priority-Tiered Modification Checklist
Not all bedroom modifications carry the same urgency or cost. This tiered framework lets you act on the highest-impact, lowest-cost changes immediately — tonight or this week — while building toward more substantial modifications over time.
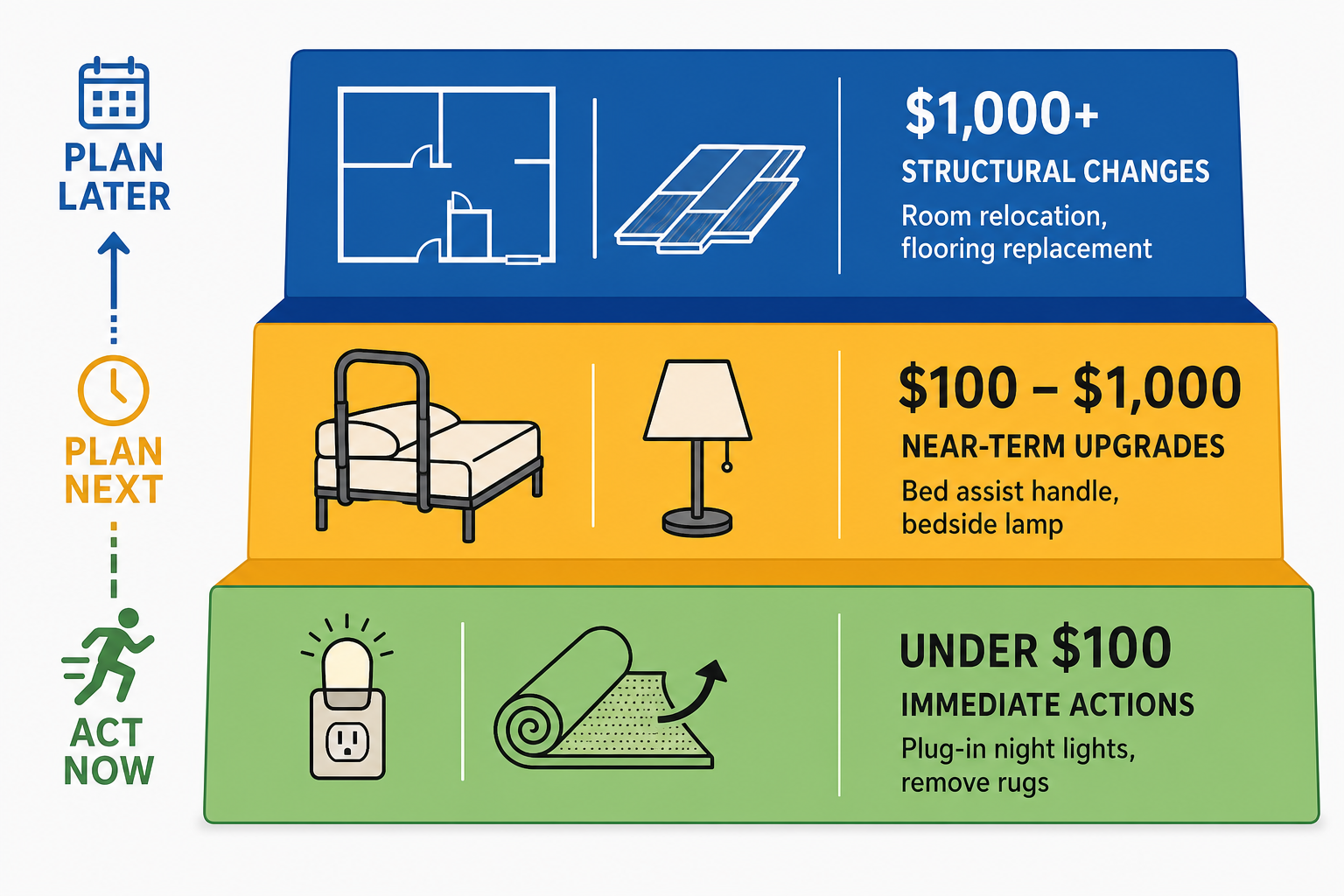
| Tier | Modification | Approximate Cost | When to Act |
|---|---|---|---|
| Tier 1 — Immediate | Motion-sensor plug-in night lights (2–3 units) | $20–$30 each | Tonight |
| Tier 1 — Immediate | Remove all throw rugs from bedroom and path to bathroom | $0 | Tonight |
| Tier 1 — Immediate | Place phone and flashlight on nightstand within arm's reach | $0–$15 | Tonight |
| Tier 1 — Immediate | Secure or reroute loose cords along baseboards | $5–$20 | This week |
| Tier 2 — Near-Term | Touch-activated bedside lamp | $25–$80 | This week |
| Tier 2 — Near-Term | Bed risers or low-profile frame to correct bed height | $20–$50 | This week |
| Tier 2 — Near-Term | Bed assist handle | $30–$60 | This week |
| Tier 2 — Near-Term | Anti-slip coating on existing flooring | ~$75 | This month |
| Tier 2 — Near-Term | Non-slip vinyl or LVP flooring (new installation) | $5–$14 per sq ft installed | This month |
| Tier 3 — Structural | Main-floor bedroom relocation | Varies widely by room conversion | Plan now, act before decline |
| Tier 3 — Structural | Adjustable bed base | $500–$2,000+ | When bed transfer is a persistent problem |
| Tier 3 — Structural | Professional flooring replacement | $5–$14 per sq ft installed | When existing flooring is a significant hazard |
Lighting the Path: Night Lights, Bedside Lamps, and Bulb Standards
Lighting is the single highest-leverage, lowest-cost category in bedroom fall prevention. The goal is not simply to have a light available — it is to have the right light in the right place, activated without requiring the person to navigate in the dark first.
Motion-sensor plug-in night lights are the foundation. Place them at floor level — not at outlet height — along the pathway from the bed to the bathroom door. The recommended spacing is every 6 to 8 feet. Floor-level placement matters because a person who has just stood from bed and is still adjusting to being upright looks downward; a light at outlet or counter height is often outside their immediate visual field. The motion-sensing function means the light activates before the person reaches it, rather than requiring them to find a switch first.
For the bedside itself, a touch-activated lamp is the safest option. It eliminates the need to locate and operate a small switch in the dark, and it can be turned on while still sitting on the edge of the bed before standing. Place it on the nightstand within arm's reach — not across the room.
For the overhead bedroom fixture, use bulbs rated at 75 to 100 watts equivalent (LED). Older adults need significantly more light than younger adults to see clearly, and standard 60-watt-equivalent bulbs are often insufficient for safe nighttime navigation. If the overhead light is on a standard switch that requires full brightness, consider adding a dimmer — a gradual increase in light is easier on eyes adjusting from complete darkness than a sudden switch to full brightness.
- Motion-sensor night lights at floor level, spaced every 6–8 feet from the bed to the bathroom door
- Touch-activated bedside lamp on the nightstand, reachable from a seated position on the bed edge
- 75–100W equivalent LED bulbs in the overhead fixture
- Dimmer switch on the overhead light for gradual brightness adjustment
- Flashlight on the nightstand as a backup for power outages — the NIA specifically recommends this as a bedroom fall prevention measure
Bed Height, Assist Handles, and Dementia-Specific Cautions
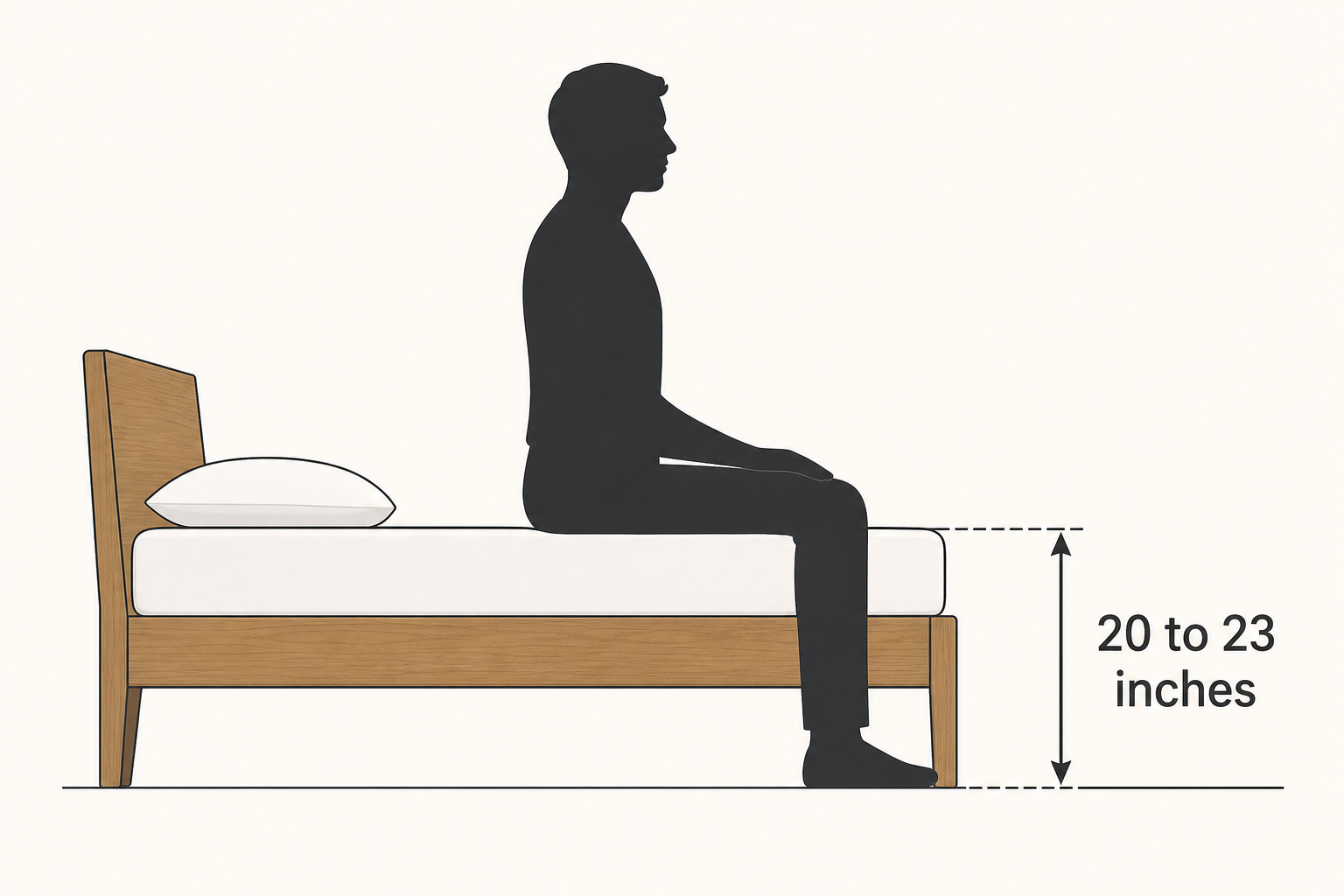
The correct bed height for most older adults is 20 to 23 inches from the floor to the top of the mattress. To check whether a bed is in this range: have the person sit on the edge of the mattress. Their feet should rest flat on the floor with their knees bent at approximately 90 degrees. If the knees are higher than the hips, the bed is too low. If the feet dangle or the person must slide to reach the floor, the bed is too high.
If the bed is too low, adjustable bed risers placed under the frame legs can raise it incrementally. Risers typically cost $20 to $30 for a set. If the bed is too high, switching to a low-profile or platform frame — which eliminates the box spring — is a common solution in the same price range.
A bed assist handle is the recommended support device for most seniors. These are L-shaped handles that insert between the mattress and box spring, providing a stable grip point for sitting up, swinging legs to the floor, and pushing to standing. They typically cost $30 to $60 and require no installation beyond sliding the base under the mattress.
For most seniors, a properly adjusted standard bed with a bed assist handle is sufficient. A hospital-style adjustable bed is not necessary unless a physician has specifically prescribed one for a medical condition. The primary goal is a stable transfer surface at the right height — which a standard bed with correct height adjustment achieves.
Flooring, Pathway Clearance, and Cord Management
The floor between the bed and the bathroom door is the most traveled path in the bedroom, and it is traveled most often in the dark. Three factors determine how safe that path is: the flooring surface itself, what is on it, and whether it is wide enough to navigate safely.
Low-pile carpet is the optimal bedroom flooring for fall prevention. It provides traction for bare feet and non-slip footwear, and it cushions the impact if a fall does occur. Tile and hardwood floors offer less friction and no cushioning. High-pile and shag carpets, despite their soft appearance, create a different hazard: the deep pile catches the legs of walkers, rollators, and shuffling feet — making them a significant trip risk for anyone using a mobility aid.
- Remove all throw rugs immediately. This is non-negotiable. Throw rugs curl at the edges, slide on smooth floors, and catch feet. No non-slip backing is fully reliable over time. The safest throw rug is no throw rug.
- Maintain a 3-foot clear path from the bed to the bathroom door. Measure it. Remove furniture, laundry baskets, shoes, or any other items that narrow the path. This width accommodates a walker or rollator and allows safe passage in the dark.
- Secure or reroute all cords. Phone chargers, lamp cords, and extension cords should run along baseboards rather than across the floor. Cord clips or cable channels (available for a few dollars at hardware stores) keep them flat and out of the walking path.
- If replacing flooring, choose non-slip vinyl or luxury vinyl plank (LVP). Installed cost runs approximately $5 to $14 per square foot nationally. For existing smooth flooring, anti-slip coating is a lower-cost option at approximately $75 for a standard bedroom.
Furniture Arrangement and Emergency Preparedness
Furniture placement in the bedroom serves two purposes: it can either obstruct the path to the bathroom or support the person moving along it. Thoughtful arrangement turns existing furniture into a balance-support system.
Place sturdy, stable furniture — a dresser, a solid chair, a low bookcase — along the bed-to-bathroom pathway where it can be used as a steadying point. The key word is sturdy: lightweight chairs, rolling office chairs, or furniture that slides easily are not safe to lean on. Furniture that is fixed, heavy, and at an appropriate height (roughly waist-level) can serve as informal balance support during nighttime trips.
The nightstand is the most important piece of furniture in the bedroom from a safety standpoint. It should hold everything the person needs to manage an emergency or a nighttime trip without getting out of bed first.
- Touch-activated lamp — so the person can turn on light before standing
- Eyeglasses — essential for safe navigation; many people forget to put them on before getting up
- Phone — for calling for help if a fall occurs
- Medical alert button — worn or placed within arm's reach; see note below
- Water — reduces the urgency of nighttime trips and supports hydration
- Flashlight — for power outages, as recommended by the National Institute on Aging
A personal emergency response system (PERS) with automatic fall detection adds an important safety layer for the bedroom specifically. If the person falls and cannot reach the phone or nightstand button, automatic fall detection can alert a monitoring center without any action required from the person on the floor. These devices are worn as a wristband or pendant. When evaluating options, look for automatic fall detection capability, two-way communication, and whether the device works both inside and outside the home. This is a category-level consideration — the right device depends on the individual's needs and living situation.
A large-print emergency information card placed on or near the nightstand is a low-cost preparedness step that is often overlooked. It should include the person's address, any medical conditions relevant to emergency responders, and the names and numbers of family contacts. In a fall scenario, the person may be disoriented or in pain — having this information immediately visible can be critical.
When to Relocate the Bedroom to the Main Floor
For seniors living in multi-story homes, relocating the bedroom to the main floor is the single highest-impact aging-in-place modification available. It eliminates stair use entirely — removing one of the most dangerous fall environments in the home from the daily routine.
This is a planning conversation, not an emergency response. The best time to discuss and execute a bedroom relocation is before a fall or before mobility declines to the point where stairs are already dangerous. Once a senior is actively struggling with stairs, the urgency and emotional difficulty of the conversation increase significantly.
Common conversion options include a den, home office, dining room, or formal living room. The key requirements are: proximity to a main-floor bathroom, enough space for the bed and a clear path to the door, and an electrical outlet configuration that supports nightstand and lamp needs. A CAPS-certified contractor can assess conversion feasibility and estimate costs.
2026 Cost Reference: Bedroom Modifications
The following cost ranges reflect 2025–2026 national installed averages based on data from MoneyGeek's home accessibility modification research. Costs in high-cost metropolitan areas typically run 20 to 40 percent higher than these national figures. Verify pricing with local contractors at the time of your project.
| Modification | DIY / Product Cost | Installed Cost Range | Notes |
|---|---|---|---|
| Motion-sensor plug-in night lights | $20–$30 each | N/A (plug-in, no installation) | Buy 2–3 for bed-to-bathroom path |
| Throw rug removal | $0 | $0 | Immediate; no cost |
| Cord management clips or channels | $5–$20 | $0 if self-installed | Hardware store |
| Flashlight for nightstand | $10–$20 | N/A | Backup for power outages |
| Touch-activated bedside lamp | $25–$80 | N/A (plug-in) | No installation needed |
| Bed risers (set of 4) | $20–$30 | N/A (no installation) | Raises bed height incrementally |
| Bed assist handle | $30–$60 | N/A (slides under mattress) | No tools required |
| Anti-slip coating on existing flooring | ~$75 (materials) | ~$75–$150 with labor | For tile or hardwood |
| Non-slip vinyl or LVP flooring | $2–$6 per sq ft (materials) | $5–$14 per sq ft installed | Full bedroom replacement |
| Grab bars (if added near bed or doorway) | $20–$100 per bar (materials) | $100–$350 per bar installed | Requires wall stud anchoring |
Funding Sources for Bedroom Modifications
Funding for bedroom modifications exists through multiple programs — but the pathways vary significantly by income, veteran status, rural location, and state of residence. Understanding which programs apply to your situation before starting a project can substantially reduce out-of-pocket costs.
| Program | Who Qualifies | Maximum Benefit | Key Notes |
|---|---|---|---|
| VA HISA Benefit | Veterans with service-connected or non-service-connected disabilities | $6,800 lifetime (service-connected); $2,000 (non-service-connected, lower rating) | Requires VA physician prescription and VA Form 10-0103. Can apply toward bedroom modifications addressing a service-connected condition. |
| VA SAH Grant | Veterans with qualifying severe service-connected disabilities | Up to $126,526 (FY2026) | For loss of multiple limbs, blindness, severe burns, or lower extremity loss post-9/11. Not available to most veterans. |
| USDA Section 504 Grant | Rural homeowners age 62+, very-low income, unable to repay a loan | Up to $10,000 ($15,000 in disaster areas) | Must be used to remove health and safety hazards. Apply through local USDA Rural Development office. |
| USDA Section 504 Loan | Rural homeowners, very-low income | Up to $40,000 at 1% fixed over 20 years | Can be combined with grant for up to $50,000 total. Income limit by county. |
| Medicaid HCBS Waivers | Medicaid-eligible individuals who meet nursing-home level of care | Varies by state and waiver program | Active in 46 states plus DC; 607,000+ on waitlists nationally (2025); average wait 32 months. Apply as early as possible. |
| HUD OAHMP | Low-income older adults, via local grantee organizations | Varies by local program | $109M awarded in FY2024 to 67 grantees. Contact local Area Agency on Aging or HUD field office. |
| ABLE Accounts | Individuals with disability onset before age 46 (expanded Jan 1, 2026) | Up to $20,000 annual contribution (2026) | Tax-advantaged savings for disability-related expenses including home modifications. Recent policy change — verify current rules. |
| Rebuilding Together | Income-eligible homeowners | Varies by local affiliate | Provides free home repairs and modifications through volunteer labor. Find local affiliate at rebuildingtogether.org. |
| Habitat for Humanity Aging in Place | Income-eligible older adult homeowners | Varies by local affiliate | Program availability varies by location. Contact local Habitat affiliate directly. |
| IRS Medical Expense Deduction | Taxpayers who itemize deductions | Deduction for costs exceeding 7.5% of AGI | Modifications for medical necessity may qualify. Consult a tax professional for individual circumstances. |
For Medicaid HCBS waivers specifically: the 32-month average wait time means that applying early — before modifications are urgently needed — is the most important step you can take. Contact your state Medicaid office or the Eldercare Locator (1-800-677-1116) to find the waiver programs available in your state and begin the application process.
Getting a Professional Assessment
For modifications beyond Tier 1, a professional assessment is worth the investment before committing to a project. Three pathways are available, each serving a different purpose.
- Occupational therapist (OT) home visit. An OT evaluates the person's specific functional limitations and identifies which modifications will have the greatest impact for that individual. This is not a generic checklist — it is a tailored assessment based on how the person actually moves through their home. A 2017 randomized controlled trial (Stark et al., cited in the 2025 PMC systematic review) found that OT-guided home modification programs reduced falls by approximately 39% in the treatment group, at an average program cost of $766 — with estimated savings of roughly $2 for every $1 spent. Some Medicaid HCBS waivers cover OT home visits; ask your physician for a referral and check with your state Medicaid program about coverage. The NIA also recommends asking a physician about an OT or physical therapist home visit following a fall.
- CAPS-certified contractor. A Certified Aging-in-Place Specialist (CAPS) is a contractor who has completed training in design solutions for aging-in-place, including budget planning, phased construction, and targeted single-room modifications. The CAPS credential, offered through the National Association of Home Builders, covers the technical and design competencies relevant to bedroom modifications. It does not guarantee outcomes or certify clinical expertise. Use a CAPS contractor for structural modifications — flooring replacement, bedroom relocation, doorway widening — where design and construction knowledge is needed. The NAHB CAPS directory allows you to search for certified contractors by location.
- AARP HomeFit Guide for self-assessment. The AARP HomeFit guide is a free room-by-room home accessibility worksheet that can serve as a starting point before engaging a professional. It helps identify modification priorities across the home, including the bedroom. Use it to organize your thinking and generate questions before an OT visit or contractor consultation — not as a substitute for professional assessment when structural modifications are planned.
Printable Bedroom Safety Checklist
Use this checklist during a bedroom safety walkthrough. Check off each item as completed. Prioritize the Tier 1 items first — they can be done immediately at minimal cost.
- ☐ Tier 1 — IMMEDIATE: Motion-sensor night lights installed at floor level along bed-to-bathroom path (one every 6–8 feet)
- ☐ Tier 1 — IMMEDIATE: All throw rugs removed from bedroom and bathroom path
- ☐ Tier 1 — IMMEDIATE: Phone placed on nightstand within arm's reach of the bed
- ☐ Tier 1 — IMMEDIATE: Flashlight on nightstand (for power outages)
- ☐ Tier 1 — IMMEDIATE: All floor cords secured or rerouted along baseboards
- ☐ Tier 1 — IMMEDIATE: Rubber-soled slippers placed beside the bed
- ☐ Tier 2 — THIS WEEK: Touch-activated lamp on nightstand
- ☐ Tier 2 — THIS WEEK: Bed height measured and adjusted to 20–23 inches (floor to mattress top)
- ☐ Tier 2 — THIS WEEK: Bed assist handle installed (slides under mattress, no tools needed)
- ☐ Tier 2 — THIS WEEK: 3-foot clear path confirmed from bed to bathroom door
- ☐ Tier 2 — THIS WEEK: Eyeglasses stored on nightstand for nighttime use
- ☐ Tier 2 — THIS WEEK: Medical alert button accessible from the bed
- ☐ Tier 2 — THIS WEEK: Large-print emergency information card placed near the bed
- ☐ Tier 2 — THIS MONTH: Overhead bulbs replaced with 75–100W equivalent LED
- ☐ Tier 2 — THIS MONTH: Anti-slip coating or new flooring assessed if current floor is tile or hardwood
- ☐ Tier 3 — PLAN NOW: Main-floor bedroom relocation discussed if home is multi-story
- ☐ Tier 3 — PLAN NOW: OT home assessment scheduled if mobility or balance has changed
- ☐ Tier 3 — PLAN NOW: Funding applications started (Medicaid HCBS waiver, VA HISA, USDA Section 504) if applicable
Frequently Asked Questions
Does Medicare cover bedroom modifications like flooring replacement or grab bar installation?
No. Standard Medicare does not cover structural bedroom modifications, including flooring replacement, grab bar installation, bedroom relocation, or assistive handle installation. Medicare Part B covers durable medical equipment — such as a prescribed hospital bed, wheelchair, or certain power mobility devices — when a physician has determined it is medically necessary. The distinction matters: if you are planning bedroom renovations, Medicare will not reimburse those costs. Funding pathways that may apply include VA benefits, Medicaid HCBS waivers, USDA Section 504 grants, and HUD OAHMP, depending on eligibility.
Are full bed rails safe for someone with dementia?
No. Full-length bed side rails carry an FDA entrapment warning for older adults, and this risk is significantly elevated for people with dementia or cognitive impairment, who may attempt to climb over or through the rail without understanding the danger. The safer approach for someone with dementia is to lower the bed to its lowest setting and place a floor mat beside the bed to cushion any falls. A bed assist handle — which provides a grip point without enclosing the sleeping area — is the safer default for most seniors. If you are considering any rail system for a person with cognitive impairment, consult with a physician or occupational therapist before installation.
How do I know if the bed is the right height?
Have the person sit on the edge of the mattress with their feet flat on the floor. Their knees should be at approximately 90 degrees — not higher than the hips, and not with feet dangling. The target range is 20 to 23 inches from the floor to the top of the mattress. If the bed is too low, adjustable bed risers (approximately $20 to $30 for a set) can raise it. If the bed is too high, switching to a low-profile or platform frame eliminates the box spring and lowers the overall height.
How long does it take to get Medicaid HCBS waiver funding for home modifications?
Medicaid HCBS waiver programs are active in 46 states plus the District of Columbia, but waitlists are long. As of 2025, more than 607,000 people are on waitlists nationally, with an average wait of approximately 32 months. This means you should apply as early as possible — ideally before modifications become urgently needed. Contact your state Medicaid office or call the Eldercare Locator at 1-800-677-1116 to identify which waiver programs are available in your state and to begin the application process. Eligibility typically requires demonstrating a need for care equivalent to nursing-home level of care.
Can a veteran use the VA HISA benefit for bedroom modifications if the disability is not service-connected?
Yes, with a lower benefit amount. The VA Home Improvements and Structural Alterations (HISA) benefit provides up to $6,800 lifetime for modifications related to a service-connected disability. For veterans with a non-service-connected condition but a lower disability rating, the benefit is up to $2,000 lifetime. In both cases, the modification must be related to the qualifying condition, and the application requires a prescription from a VA physician and submission of VA Form 10-0103 through a VA medical facility. Contact your local VA medical center's prosthetics or social work department to begin the process.
What is the first modification I should make tonight?
Remove all throw rugs from the bedroom and the path to the bathroom, and install motion-sensor plug-in night lights at floor level along that path. These two actions address the most common mechanisms of bedroom falls — trip hazards and darkness during nighttime bathroom trips — and can be completed for under $50 in under an hour. If you can only do one thing tonight, remove the throw rugs. They cost nothing to remove and eliminate a significant hazard immediately.
Does my parent need a hospital bed?
For most older adults aging at home, a hospital-style adjustable bed is not necessary. A standard bed adjusted to the correct height (20 to 23 inches, floor to mattress top) with a bed assist handle provides a safe and comfortable sleeping environment for the majority of seniors. A hospital bed may be appropriate when a physician prescribes one for a specific medical condition — for example, when head-of-bed elevation is medically required, or when a person needs frequent repositioning due to a medical condition. In those cases, Medicare Part B may cover a prescribed hospital bed as durable medical equipment. If you are uncertain whether a hospital bed is needed, ask the person's physician or request an occupational therapy assessment.
How effective are home modifications at actually preventing falls?
The evidence is strong. A 2025 systematic review of 20 home modification studies found that 65% of the studies confirmed effectiveness in fall prevention, functional independence, or cost savings. The most rigorous evidence comes from a randomized controlled trial (Stark et al., 2017) in which an occupational therapist-guided modification program reduced falls by approximately 39% in the experimental group, with 80% of participants adhering to the recommended modifications. The average program cost was $766 per person, with estimated savings of approximately $2 for every $1 spent when accounting for reduced fall-related healthcare costs. These findings apply to professionally guided modification programs — self-directed modifications without assessment may achieve more modest results, which is one reason a professional OT assessment is recommended before undertaking structural changes.
Related reading
- How Much Does a CAPS Specialist Cost? A Family Budget Guide for Home Modifications
- Funding Sources for Home Modifications: A Complete Guide to VA, Medicaid, Grants, and More
- Hidden Disparities in Bathroom Safety: Why Non-Hispanic Black and Hispanic Seniors Are Far Less Likely to Have Bathroom Modifications — and What Caregivers Can Do
Need a professional assessment?
Find a CAPS-credentialed professional or local aging services through our outbound resource list — we never name or rank individual contractors.
Find Local HelpNoticed something outdated or inaccurate on this page? Flag a correction. We review every report against CDC, NIA, and AARP HomeFit guidance before updating a page.