
Caregiver decision guide
Walker vs. Rollator: A Clinical Decision Guide for Seniors and Caregivers
Choosing the right mobility aid—walker or rollator—depends on three clinical factors: weight-bearing need, balance control, and grip strength. This guide helps adult children and caregivers match the device to the senior's mobility profile to prevent falls and support independence.
Why the Wrong Choice Leads to Falls

Every year, more than 14 million older adults — roughly one in four people age 65 and older — report falling, according to the CDC. The age-adjusted fall death rate climbed 21% between 2018 and 2024, a stark reminder that falls are not an inevitable part of aging. Many of these falls are preventable, and choosing the right mobility aid is one of the most direct prevention strategies available to families.
Yet the decision between a standard walker and a rollator is too often driven by appearance, cost, or convenience rather than by the senior’s actual physical needs. A rollator handed to someone who cannot reliably squeeze its brakes or who needs to bear weight through their arms can turn a supportive device into a hazard. Conversely, a standard walker that forces a person to stoop and shuffle can discourage walking altogether. The core thesis of this guide is straightforward: the walker-versus-rollator decision hinges on three clinically validated factors — weight-bearing need, balance control, and grip strength. Matching the device to the person’s actual mobility profile prevents falls and extends independent walking.
How Walkers Work and Who They Fit
A standard walker — four legs with rubber tips, no wheels — is the most stable walking aid available. It provides a solid base of support and can bear up to roughly 50% of the user’s body weight, according to ThedaCare’s mobility aid guidelines. This makes it the safest option for anyone with significant balance issues, bilateral weakness (both legs affected), or recovery needs after hip or knee surgery. Variants include the two-wheel walker (front wheels, rear glides) for those who can take some weight but struggle to lift the device, and the knee walker for foot or ankle injuries.
The key operational rule for a standard walker: you lift it, then step into it. The Mayo Clinic emphasizes that walkers should not be pushed ahead of the user. Lift the walker forward a short distance, place it firmly on all four legs, and then step inside the frame. This “step-into” pattern provides maximum stability and is essential for users who need to hop, shuffle, or take one step at a time.
How Rollators Work and Who They Fit
Rollators are four-wheeled walkers equipped with hand brakes, a built-in seat, and often a storage pouch or basket. They are designed for people who have enough balance and endurance to walk continuously but need a place to rest periodically, help carrying items, or a gentle boost in confidence for longer outings. A systematic review of 18 studies published in PMC found that rollator users preserve natural gait symmetry patterns better than cane or walker users, and frequent users show increased gait velocity and stride length. However, first-time users did not improve immediately — training is critical.
Rollators are not for everyone. Because they roll freely, they require reliable hand strength to operate the brakes and enough balance to control the device’s direction, especially on uneven ground. The brake mechanism slows the device but does not lock it completely — the wheels can still move even with brakes applied. An occupational therapist writing for AskSAMIE warns that a rollator is unsuitable for anyone who needs to lean heavily on the device or who cannot squeeze the brake levers without fatiguing.
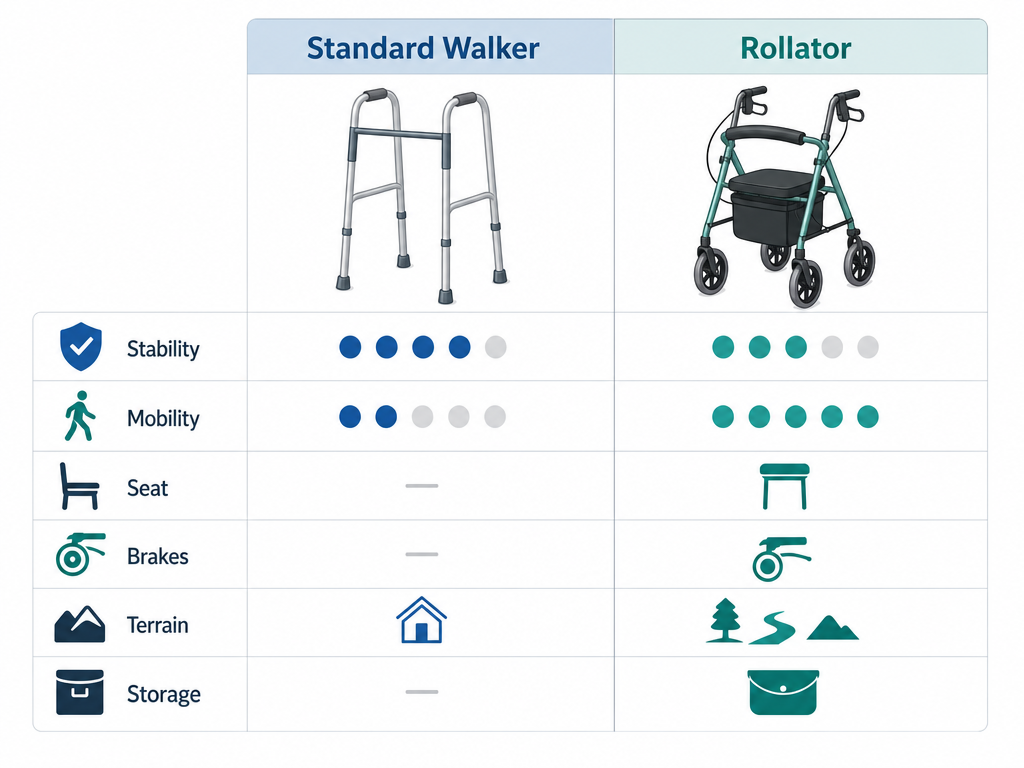
Side-by-Side Decision Matrix
| Feature | Standard Walker | Rollator |
|---|---|---|
| Stability | Highest — four fixed legs provide a rigid base | Lower — wheels can move even with brakes locked |
| Weight-bearing support | Up to ~50% of body weight (based on clinical observation) | Minimal — user should not lean heavily on the device |
| Mobility / Speed | Slow — must be lifted and placed for each step | Faster — wheels allow continuous gliding |
| Built-in seat | Not standard; some models add a seat as accessory | Yes — allows resting during long walks |
| Brake type | None | Hand brakes; require sufficient grip strength |
| Terrain suitability | Indoor, flat surfaces best | Indoor and outdoor; handles curbs and rough ground better |
| Storage / carrying | Minimal; optional basket or pouch | Typically includes storage pouch or basket |
Three-Question Clinical Self-Check
Use these three questions to start narrowing down the choice. Answer each honestly based on the senior's current condition — not on what they did last year or what might be true after rehab.
- Can the user bear weight through their arms and shoulders? If yes, a standard walker is possible. If no (weak arms, arthritis, injury), a walker that requires lifting may be too demanding, and a rollator (which requires less arm strength) or a front‑wheeled walker should be considered.
- Can the user reliably squeeze brake levers? Rollators require both grip strength and endurance to slow the device on slopes and to lock it when seated. If the user cannot depress the levers fully or fatigue quickly, a rollator is unsafe.
- Does the user need a seat for rest during walks? If the person can walk continuously for 20–30 minutes without needing to sit, a walker may suffice. If they need frequent rests (due to fatigue, heart condition, or breathing difficulty), a rollator’s built‑in seat is a major safety advantage.
Proper Fit Guide: Getting the Height Right
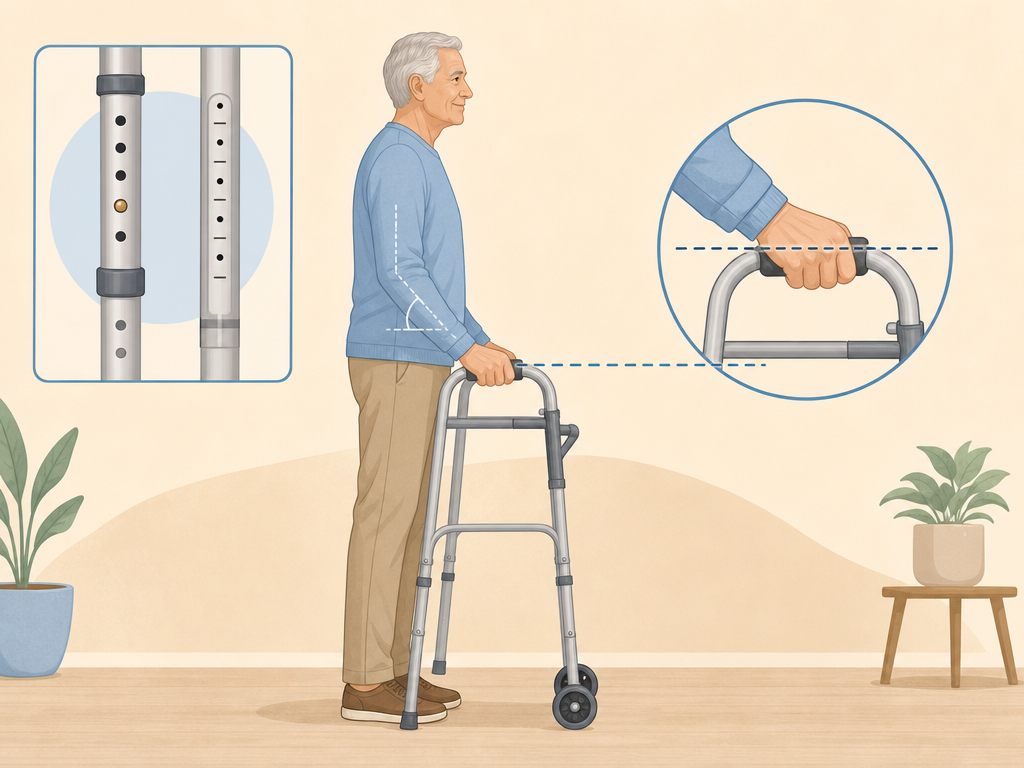
An improperly adjusted walker or rollator is uncomfortable and dangerous. The Mayo Clinic’s fitting rule is simple: the top of the grip should line up with the crease of the wrist when the user stands with arms hanging relaxed at their sides. When the hands rest on the grips, the elbows should bend at a comfortable angle of about 15 degrees — enough to allow arm swing and prevent slouching. If the device is too low, the user will hunch over; if too high, they cannot push down effectively and may lose balance.
Most standard walkers and rollators have adjustable height legs. Measure from the floor to the user’s wrist crease while the person stands in walking shoes on a flat surface. Test the fit by having the user stand inside the walker with hands on the grips — they should be able to stand upright without leaning forward or to the side. Also check the device’s weight capacity: most standard models support 250–350 pounds, but heavy-duty versions are available. Never exceed the manufacturer’s limit.
Medicare Coverage for Walkers and Rollators
Both walkers and rollators are classified as Durable Medical Equipment (DME) under Medicare Part B. Medicare will cover the cost when a doctor prescribes the device as medically necessary for use in the home. According to Medicare.gov, after the Part B deductible is met, the beneficiary pays 20% of the Medicare-approved amount as coinsurance. The supplier must accept assignment to keep out-of-pocket costs at this level.
To avoid surprises, confirm that the supplier is a Medicare-enrolled DME provider and that the prescription specifies the type of walker or rollator needed. Medicare does not cover accessories like baskets or pouches unless they are integral to the device’s function. Some Medicare Advantage plans may have different rules — always check with the plan directly.
When to Consult a Physical Therapist
This guide provides a framework, but it cannot replace a hands-on clinical evaluation. A physical therapist (PT) can assess balance, gait, strength, and endurance — the raw data that determines which mobility aid is safe and effective for an individual. This is especially important for seniors with a history of falls, neurological conditions like Parkinson’s or stroke, arthritis in the hands or shoulders, or complex health issues that affect multiple systems.
A typical PT mobility aid assessment includes:
- Balance testing (static and dynamic, with and without the device)
- Gait analysis (walking speed, step length, symmetry, stability)
- Strength testing of upper and lower extremities
- Grip strength and endurance assessment
- Device trial (testing multiple models in a controlled environment)
- Training on proper use, transfer techniques, and safety maneuvers
Questions to bring to a clinician or OT
This is not medical, legal, or a family's final decision — only a framework. Bring these questions to a clinician, occupational therapist, or your local Area Agency on Aging.
Find Local HelpRelated reading
Noticed something outdated or inaccurate on this page? Flag a correction. We review every report against CDC, NIA, and AARP HomeFit guidance before updating a page.