Geriatrician vs. PCP: How to Know Which Primary Care Provider Is Right for Your Aging Parent
A practical decision guide for adult children trying to determine whether their aging parent should switch to a geriatrician, stay with their family PCP, or use a hybrid approach — based on health complexity, medication count, and functional status, not age alone.
By Editorial Team
geriatrician
primary care
healthcare coordination
adult children
new caregiver
📄
A printable version of this guide is available. Use your browser's print function (Ctrl+P / ⌘P) to save or print.
Why This Decision Matters Now
If you are an adult child in your 40s or 50s who has recently taken on a larger role in a parent's healthcare, you have likely run into a question that feels deceptively simple: Should Mom or Dad switch to a geriatrician, or stick with the family doctor they have seen for years? The answer is not as straightforward as it sounds, and the stakes are higher than most families realize.
Between 2000 and 2022, the U.S. population of adults aged 65 and older grew by 60%. Over that same period, the number of board-certified geriatricians dropped by 28%, according to data cited by the American Medical Association. Today, the American Geriatrics Society (AGS) estimates there are fewer than 7,000 geriatricians in the entire country — roughly one for every 10,000 older adults. The Health Resources and Services Administration (HRSA) projects a further shortage of 1,740 geriatricians by 2036, alongside a broader shortfall of 70,610 primary care physicians by 2038.
Meanwhile, a September 2024 survey by The John A. Hartford Foundation and Age Wave found that 82% of older adults say the U.S. healthcare system is not prepared for the growing aging population. Only 58% of older adults with a provider say their providers ask about what matters to them. Only 40% say providers routinely evaluate cognitive health, and 55% say providers evaluate mobility.
If you are still getting your bearings as a caregiver, our stage-based guide for new caregivers can help you build a foundation before diving into provider decisions.
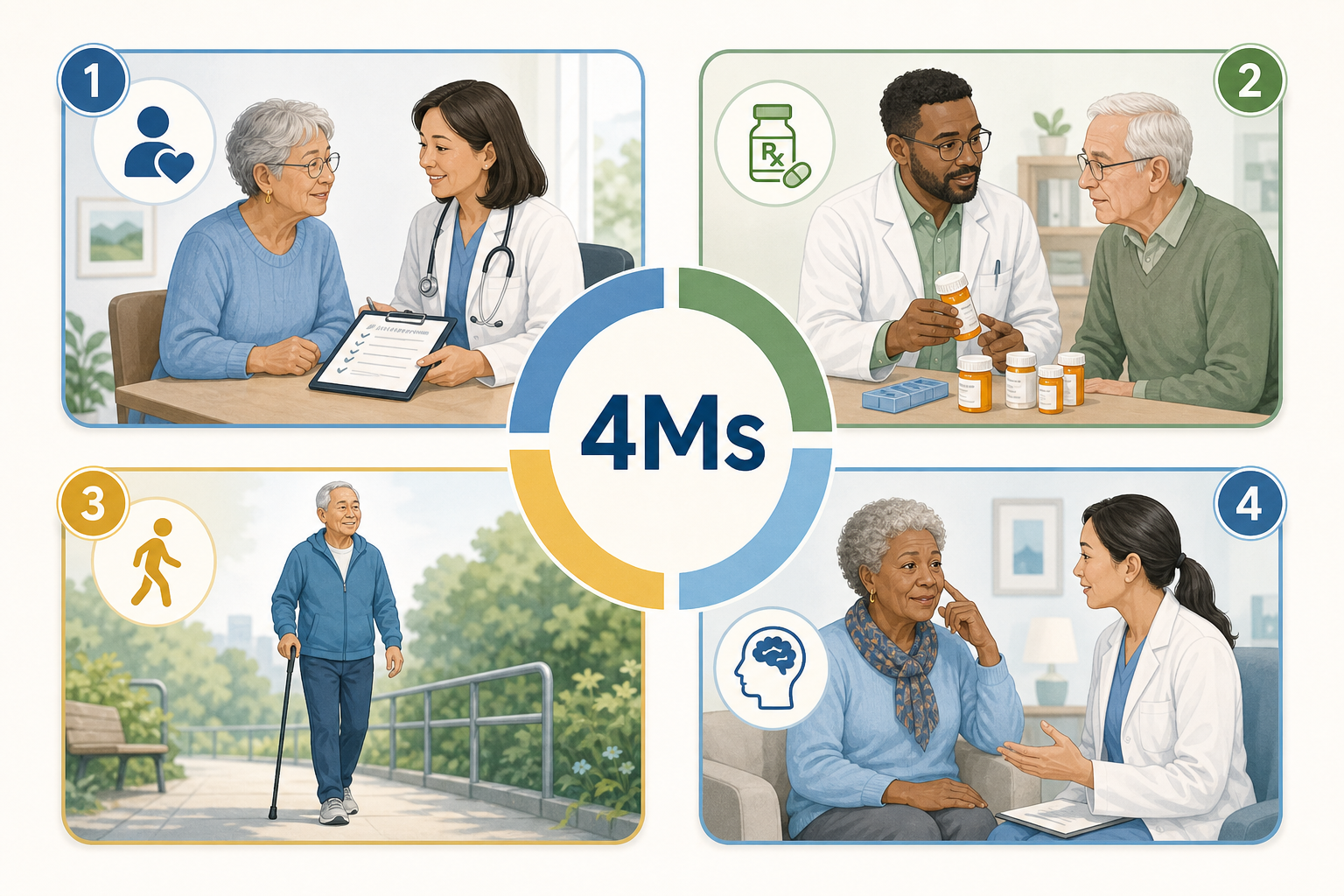
What a Geriatrician Does Differently: The 4Ms Framework
A geriatrician is a primary care doctor who has completed a residency in family or internal medicine plus an additional one to two years of fellowship training specifically focused on the care of older adults. That extra training changes how they approach a patient. Instead of treating each disease in isolation — heart failure here, osteoporosis there — a geriatrician looks at the whole person through a lens called the 4Ms Framework, which is endorsed by the Centers for Medicare & Medicaid Services (CMS) and developed by the John A. Hartford Foundation and the Institute for Healthcare Improvement.
The 4Ms Framework guides geriatricians to focus on what matters most to the patient, not just their diagnoses.
The 4Ms Framework: How geriatricians approach care differently than a disease-focused model.
4M Domain
What It Means in Practice
What Matters
Aligning care with the patient's own goals and preferences — not just clinical targets. Only 58% of older adults say their providers ask about what matters to them (John A. Hartford Foundation, 2024).
Medication
Reviewing every prescription for necessity, dosage, and interaction risk. Polypharmacy (5+ medications) is a primary trigger for geriatric referral.
Mobility
Assessing gait, balance, and strength to prevent falls and preserve independence. 55% of older adults say providers do not routinely evaluate mobility.
Mentation
Screening for cognitive decline, depression, and delirium — conditions that standard PCP visits often miss. Only 40% of older adults say providers routinely evaluate cognitive health.
The training gap is stark. According to the John A. Hartford Foundation, only 10% of U.S. medical schools require a rotation in geriatric care, compared to 96% that require a rotation in pediatrics. This means most family doctors and internists enter practice with minimal formal training in the conditions that will define their older patients' quality of life.
When to Stay With Your Parent's Current PCP
Not every older adult needs a geriatrician. In fact, most seniors in generally good health are well served by a primary care provider who knows their history and has an established relationship with them. WebMD notes that many older adults do not need a geriatrician if they are in generally good health, managing only one or two medications, and have a strong rapport with their current doctor.
AgingCare.com reinforces this: seniors without serious health problems often stay with their PCP due to the value of an established relationship. The doctor knows the patient's medical history, personality, and family context — and that continuity of care has real value.
Your parent has one or two stable chronic conditions (e.g., well-controlled hypertension, mild arthritis)
They take fewer than five medications and have not experienced adverse drug reactions
They are cognitively intact with no concerns about memory or judgment
They are mobile and independent in basic activities of daily living (bathing, dressing, eating, transferring)
They have not had a fall, hospitalization, or emergency department visit in the past year
The PCP communicates well with you as the caregiver and is responsive to questions
When to Add or Switch to a Geriatrician
The decision to involve a geriatrician should be driven by complexity, not a birthday. WebMD and AgingCare both identify specific triggers that signal it is time to consider a geriatrician. The American Medical Association adds that geriatricians are uniquely equipped to manage the interplay of multiple chronic conditions, medications, and functional decline.
Six triggers that suggest it is time to add or switch to a geriatrician.
Trigger
Why It Matters
What a Geriatrician Can Do
3 or more chronic conditions
Conditions like heart failure, diabetes, osteoporosis, and COPD interact in ways that disease-specific specialists may miss.
Conduct a comprehensive geriatric assessment that evaluates how conditions affect each other and the patient's overall function.
The Hybrid Option: Periodic Geriatric Consultation
Given the severe shortage of geriatricians — fewer than 7,000 nationwide — many families cannot find a geriatrician who is accepting new patients for ongoing primary care. Even when they can, switching providers is disruptive, especially for an older adult who trusts their current doctor.
WebMD describes a practical third path: keep your parent's PCP for ongoing care but schedule a one-time or periodic geriatric consultation. This hybrid approach gives you the best of both worlds. The geriatrician performs a comprehensive assessment — medication review, cognitive screening, mobility evaluation, and care goal alignment — and then sends a detailed report back to the PCP, who continues to manage day-to-day care.
This approach is especially practical for families who live in areas without a geriatrician accepting new patients. Telehealth geriatric consultations are increasingly available through academic medical centers and hospital-affiliated geriatric clinics, making the hybrid option accessible even in rural or underserved regions.
Practical Questions to Ask When Evaluating a Provider
Whether you are evaluating a PCP or a geriatrician, you need a structured way to assess whether the provider is a good fit for your parent's needs. The National Institute on Aging (NIA) offers a validated framework of 17 questions organized into four categories. ArchWell Health provides a complementary set of 10 caregiver-focused questions designed specifically for adult children attending appointments with a parent.
Key questions to ask when evaluating a primary care provider for an aging parent, adapted from the NIA's 17-question framework and ArchWell Health's caregiver-focused questions.
Category
Key Questions to Ask
Basics & Access
Are you accepting new patients? Do you accept Medicare assignment? What is the typical wait time for a new patient appointment? How long are routine appointments (15 minutes vs. 30+ minutes)?
Geriatric Expertise
Do you have additional training or certification in geriatrics? How many older adults with complex conditions do you see? Do you routinely screen for cognitive impairment, fall risk, and depression?
Care Coordination
Who handles after-hours calls? How do you communicate with specialists? Do you have a care coordinator or social worker on staff? How do you involve family caregivers in care planning?
Medication Management
Do you conduct a comprehensive medication review at every visit? How do you approach deprescribing? Are you familiar with the Beers Criteria for potentially inappropriate medications in older adults?
Functional & Cognitive Assessment
Do you assess mobility and fall risk at routine visits? Do you perform cognitive screening? What is your process if a screening reveals a concern?
ArchWell Health's 2025 guide specifically recommends asking: What is the goal of their care plan? What lifestyle changes could help? What are the side effects of their medications? When should we set up a long-term care plan? What local resources are available? What changes in health should I watch for? These questions shift the conversation from reactive treatment to proactive planning.
How to Find a Geriatrician Given the Nationwide Shortage
The practical barrier is real. With fewer than 7,000 geriatricians in the U.S. and a projected shortage of 1,740 by 2036 (HRSA), many families will struggle to find one within a reasonable distance. The AGS projects the country will need more than 23,000 geriatricians by 2030 to meet demand — a number that current training pipelines cannot come close to producing.
Here are actionable strategies for finding a geriatrician or geriatric-level care:
Use the AGS Find a Geriatrician online directory. It is the most comprehensive national listing, though it may not include every provider.
Search hospital-affiliated geriatric clinics. Many academic medical centers and large health systems have geriatric medicine departments that offer both primary care and consultation services.
Consider telehealth geriatric consultations. Several academic medical centers now offer remote geriatric assessments, which can be especially valuable for families in rural or nonmetro areas — where HRSA projects a 39% shortage of primary care physicians by 2038.
Look for geriatric nurse practitioners or physician assistants. Many geriatric practices are staffed by advanced practice providers who work under a geriatrician's supervision and deliver the same 4Ms-based care.
Ask your parent's current PCP for a referral. Even if the PCP cannot name a specific geriatrician, they may know which local health systems have geriatric programs.
Check with your Area Agency on Aging. These local organizations often maintain lists of geriatric providers and can help with transportation and scheduling logistics.
The decision between staying with a PCP, adding a geriatric consultation, or switching to a geriatrician is not a binary choice. It is a spectrum that depends on your parent's current health complexity, medication burden, and functional status — and it may change over time.
Decision flowchart: Three pathways for primary care for seniors based on health complexity, medication count, and functional status.
Three scenarios and the recommended primary care path for each.
Scenario
Recommended Path
Key Considerations
Generally healthy, 1–2 medications, stable chronic conditions, strong PCP relationship
Stay with current PCP
Ensure annual wellness visits include cognitive and mobility screening. Reassess if condition changes.
Emerging complexity: new diagnosis, first cognitive concern, medication creep (3–4 meds), or a recent fall
Add a one-time geriatric consultation
Keep PCP for ongoing care. Use the consultation for a comprehensive baseline assessment and care plan update.
The most important takeaway is this: the decision is not about age. It is about complexity. A 68-year-old with well-controlled hypertension and no other issues does not need a geriatrician. A 72-year-old with heart failure, diabetes, mild cognitive impairment, and eight medications needs more than a standard 15-minute PCP visit can provide. Know the triggers, ask the right questions, and do not be afraid to use the hybrid option when a full switch is not possible.


Comments
Join the discussion with an anonymous comment.