The Essential Guide to Home Care Services for the Elderly
15 minutesReviewed: 2026-07-09
The Essential Guide to Home Care Services for the Elderly
This comprehensive guide explains the types of home care services for the elderly, the critical distinction between home care and home health care, 2026 costs, payment options, and how to choose a provider — helping families make informed decisions when a parent needs help at home.
By Editorial Team
new caregiver
experienced caregiver
long-distance caregiving
spousal caregiver
working caregiver
daily routines
medication management
personal hygiene
care coordination
first steps
ADLs
IADLs
When a family says, “We think Dad needs home care,” the next sentence matters more than most people realize. Does he need someone to make lunch, drive him to appointments, and notice whether the mail is piling up? Does he need help bathing and getting safely to the toilet? Or does he need wound care, injections, therapy, or nursing assessment after a hospital stay?
Those are not small wording differences. They point to different workers, different prices, and different payment rules. The National Institute on Aging describes services at home as a broad mix that can include help with personal care, household tasks, meals, transportation, money management, and health care; Johns Hopkins separately describes home health care as medically oriented care that may include nursing, therapy, social work, and home health aide services under a physician-directed plan.[1][2]
Many families start this search before they have the right vocabulary. That is understandable. A parent has lost weight, stopped driving at night, skipped pills, fallen once, or started wearing the same clothes for several days. Everyone is worried. But if the first phone call asks for “a nurse” when the need is really bathing help and meal preparation, the family may overpay, call the wrong provider, or expect Medicare to cover something Medicare generally does not cover.
The wish to stay home is not rare. A 2026 Pew Research Center analysis found that 82% of older adults want to age in place.[3] That number is meaningful only if families can translate “staying home” into a workable care plan: what help is needed, who is allowed to provide it, how many hours a week are realistic, and which payer, if any, matches that kind of care.
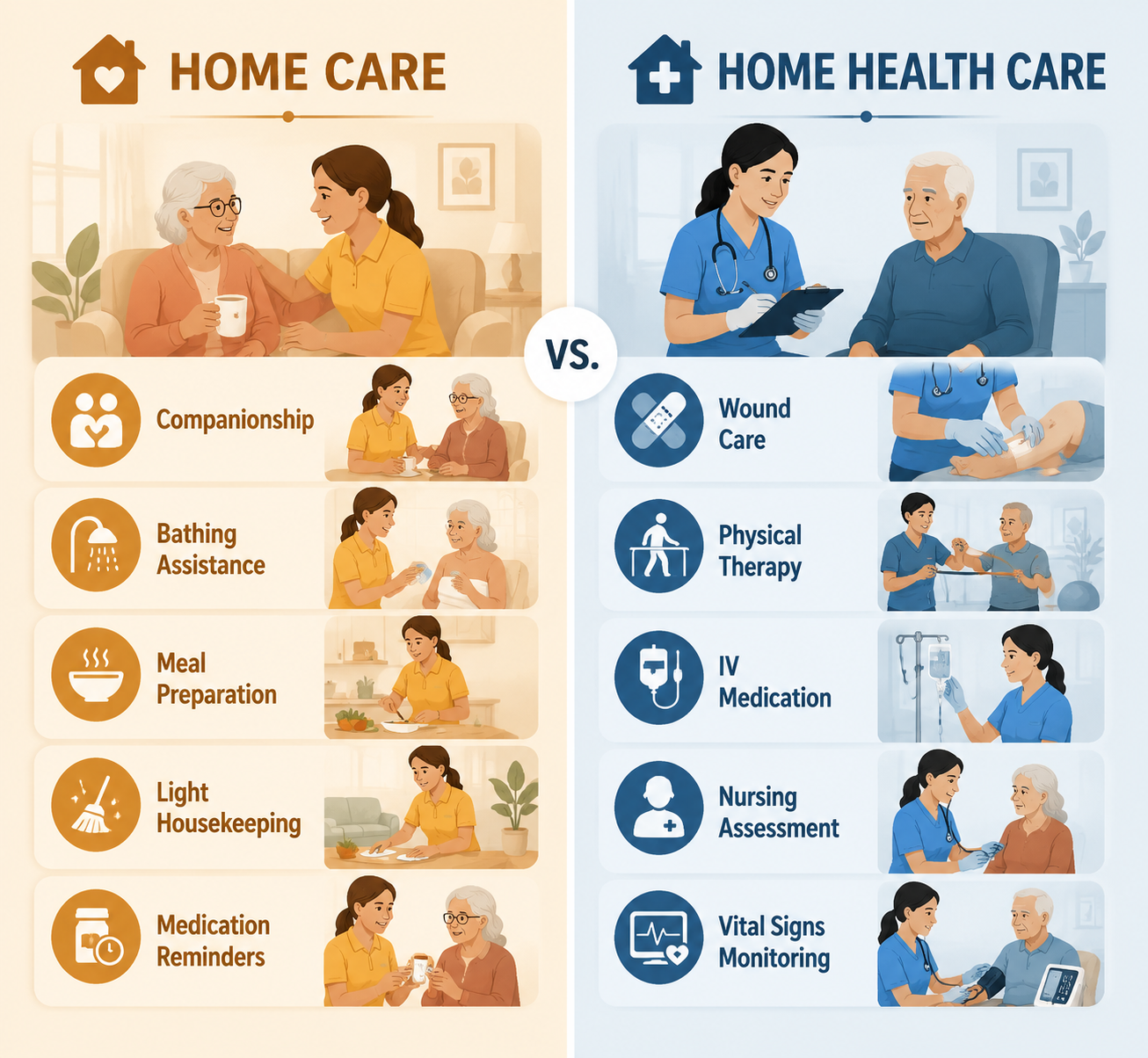
Home Care and Home Health Care Are Not the Same Service
For most families, the first useful split is this: home care is usually nonmedical help with daily life, while home health care is skilled or medically directed care provided at home.
Often private pay unless Medicaid waiver, VA benefit, long-term care insurance, or local program applies
Wound care, injections, skilled nursing assessment, physical therapy, occupational therapy, speech therapy after illness or injury
Home health care
May be covered by Medicare when eligibility rules are met
Comfort care for a terminal illness, symptom management, family support, spiritual or social work support
Hospice care at home
May be covered under a hospice benefit when eligibility rules are met
Medicare’s boundary belongs near the beginning of this discussion, not hidden in the fine print. Medicare covers eligible home health services when a person needs part-time or intermittent skilled care and is homebound under Medicare rules; it does not cover 24-hour-a-day care at home, meals delivered to the home, homemaker services unrelated to the care plan, or personal care when that is the only care needed.[4]
That does not make nonmedical care less important. The person who helps with a shower may be the first one to see a new bruise. The aide making breakfast may notice spoiled food, unpaid bills, confusion with pill bottles, or a change in how a parent walks. This work is practical, intimate, and often protective. It is just not the same as skilled nursing.
If you want a deeper side-by-side explanation, see our guide to home care vs. home health care. For now, keep the distinction in view because nearly every later decision depends on it.
What Home Care Services for Elderly Adults Usually Include
Home care services for elderly adults are best understood by the task being performed, not by the warm label on the brochure. A caregiver may spend one visit playing cards and preparing lunch, and another visit helping someone transfer from bed to chair. Those are different levels of responsibility, even when the same agency coordinates them.
Companion Care
Companion care is for isolation, light supervision, routine, and social support. A companion may visit, read mail aloud, play games, go for walks, accompany a parent to an appointment, or make sure someone eats lunch. This can be enough when the parent is physically able to bathe, dress, toilet, and move around safely but is becoming withdrawn or needs another adult in the house for part of the day.
Homemaker Help
Homemaker services focus on the home staying livable: laundry, light housekeeping, grocery shopping, meal preparation, changing bed linens, and basic errands. The National Institute on Aging includes household chores, meals, and transportation among the supports that can help older adults remain at home.[1]
This is often the right category when the refrigerator is empty, the bathroom is no longer being cleaned, or bills and mail are accumulating. It is not the same as medical care, and it is not automatically covered by health insurance.
Personal Care and ADL Help
Personal care is where families need to be especially plain. If a parent needs help bathing, dressing, toileting, transferring, grooming, eating, or walking safely, say so. These are activities of daily living, often shortened to ADLs. They are more hands-on than companionship or homemaker help, and they require a caregiver who is trained and allowed by state rules and agency policy to assist with body care.
Medication is another place where language matters. “Medication reminders” usually means prompting the person to take medicine that has already been set up. It is different from medication administration, injections, medication reconciliation, or clinical judgment about side effects. If the pillbox is confusing, prescriptions have changed after a hospital stay, or doses are being missed in a way that creates medical risk, ask whether a nurse needs to review the situation.
Respite Care
Respite care gives the family caregiver time away while another trained person provides supervision or hands-on help. It may be a few hours a week, a regular day each weekend, or a temporary block after surgery or during caregiver burnout. The service itself may look like companion care, homemaker help, or personal care; what makes it respite is that it is deliberately protecting the family caregiver’s ability to continue.
Skilled Nursing and Therapy at Home
Skilled home health care may include nursing care, physical therapy, occupational therapy, speech therapy, medical social services, or aide services tied to a skilled plan of care. Johns Hopkins lists nursing, therapy, medical social work, home health aide support, homemaker or basic assistance care, companionship, volunteer care, nutritional support, laboratory and imaging services, pharmaceutical services, transportation, and home-delivered meals as possible types of services associated with care at home, while distinguishing the clinical roles involved.[2]
A parent discharged after a stroke, hip fracture, infection, wound, or new diagnosis may need this level temporarily. The provider, billing, documentation, and oversight are different from hiring someone privately to help with showers three mornings a week.
Hospice Care at Home
Hospice is not simply “more home care.” It is comfort-focused care for someone with a terminal illness who meets eligibility criteria. Hospice may bring nursing, aides, social work, spiritual care, medications related to comfort, equipment, and family support into the home. It does not mean the family has 24-hour bedside staffing by default, so families still need to ask what visits are included and what help is available after hours.
Match the Need to the Worker, Not the Other Way Around
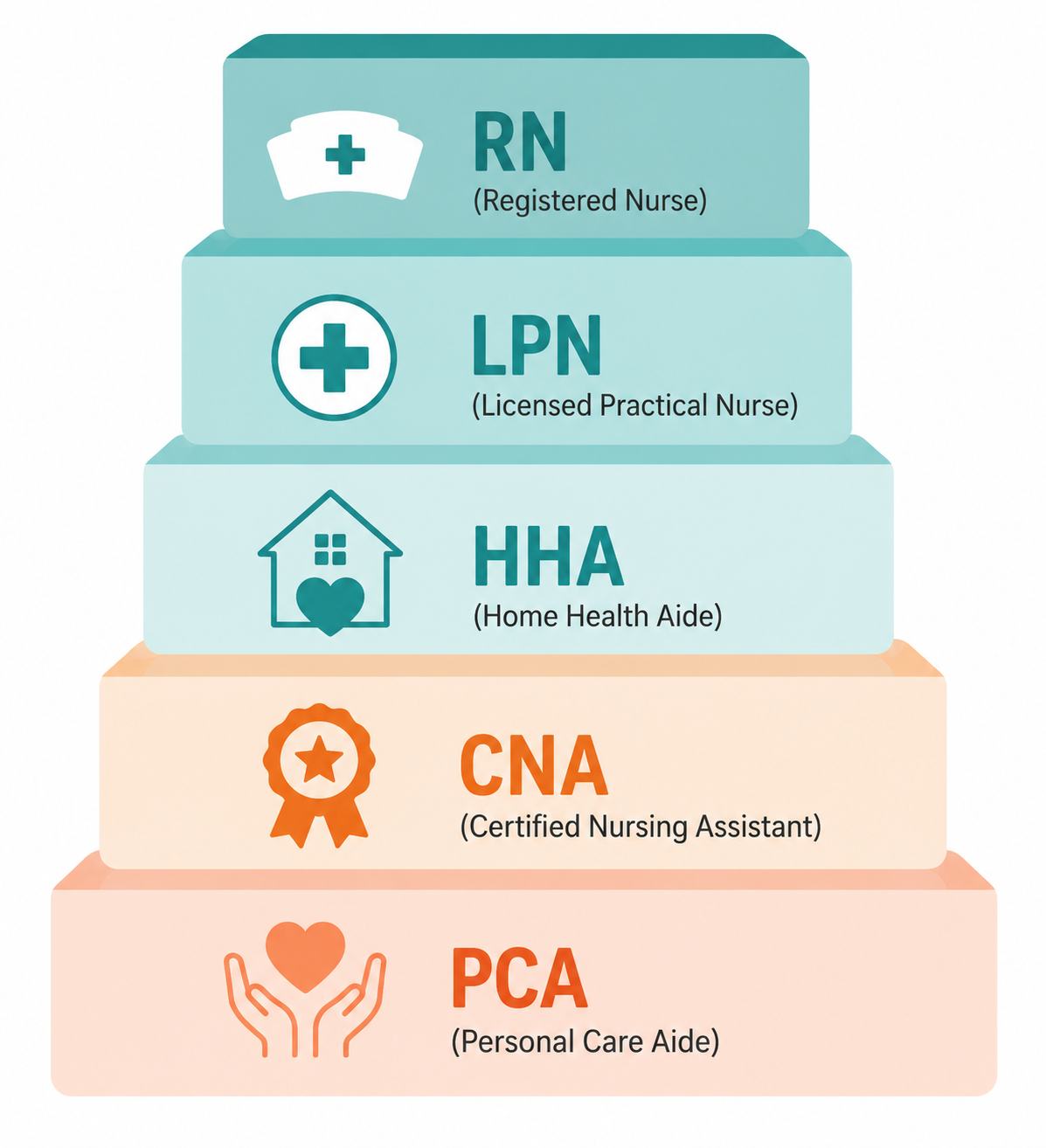
Families often ask for a “caregiver” as if that word tells an agency enough. It does not. A caregiver may be a private companion, a personal care aide, a certified nursing assistant, a home health aide, a licensed practical nurse, or a registered nurse. The titles overlap in everyday speech, but they do not carry the same training, scope, supervision, or price.
Credential or role
Commonly appropriate for
Important limits to ask about
PCA: Personal Care Aide
Companionship, homemaker help, errands, meal preparation, reminders, and hands-on personal care where allowed
Usually not licensed for skilled nursing tasks; training and allowed duties vary by state and employer
Works under supervision; generally does not provide independent nursing assessment or skilled treatment
HHA: Home Health Aide
Personal care in a home health context, often supporting a skilled plan of care
Duties depend on state rules, agency policy, and whether services are part of a certified home health episode
LPN/LVN: Licensed Practical or Vocational Nurse
Certain nursing tasks, medication-related duties, wound care support, and monitoring under RN or physician direction
Scope varies by state; not the same as an RN assessment role
RN: Registered Nurse
Assessment, care planning, skilled nursing judgment, medication teaching, wound assessment, and coordination with clinicians
Usually more costly and not necessary for routine custodial help alone
AARP’s caregiving guidance distinguishes among informal caregivers, personal care aides, home health aides, certified nursing assistants, licensed practical nurses, and registered nurses when helping families decide whom to hire.[5] CaringInfo similarly separates in-home caregiver types by role, from companions and homemakers to personal care aides, home health aides, nurses, and therapists.[6]
The practical question is not “Who has the most advanced title?” It is “What must be done safely in the home this week?” A parent who is lonely and no longer cooks may need a companion or homemaker. A parent who cannot shower without steadying assistance needs personal care. A parent with a new wound, unstable symptoms, or a complicated medication change may need a nurse involved, even if an aide is still doing the daily bathing help.
When calling an agency, describe the tasks instead of starting with a job title. Say, “My mother needs help getting in and out of the shower, changing clothes, preparing lunch, and remembering morning pills.” Or, “My father was discharged with a wound and new medications, and we need to know whether skilled home health is appropriate.” Those two calls should not be routed the same way.
If the task involves company, meals, errands, light housekeeping, or reminders, start with companion, homemaker, or PCA-level home care.
If the task involves bathing, dressing, toileting, transfers, or feeding, ask for personal care and clarify what training the aide has.
If the task involves wounds, injections, unstable symptoms, medication changes, therapy, or clinical assessment, ask whether skilled home health or nursing is needed.
If the main issue is caregiver exhaustion, ask about respite care and be specific about whether the respite worker must provide hands-on ADL help.
Safety issues may sit beside, but not inside, this decision. If the parent’s main problem is repeated falls, start with a fall prevention plan. If the house itself is the obstacle, look at home modifications. If the family is trying to check in from a distance, compare monitoring technology. If dementia behaviors are driving the need, route the care plan through memory care guidance rather than treating every problem as a staffing problem.
What Home Care Costs in 2026
In 2026, A Place for Mom reports a national median in-home care cost of $34 per hour.[7] SeniorLiving.org’s 2026 cost data places the national hourly figure at $35 and shows state-level variation from about $25 per hour in Mississippi to about $44 per hour in South Dakota.[8] Those figures are close enough to be useful for planning, but they are not interchangeable; cost sources use their own data collection methods, markets, and definitions, so compare numbers from the same source when building a state-by-state estimate.
The hourly rate is only the first line of the budget. The real bill comes from hours, minimum shifts, weekend rates, overnight rates, caregiver credentials, agency fees, and whether the parent needs standby supervision or hands-on help.
Weekly schedule
At $34/hour
At $35/hour
What this often means in real life
6 hours/week
$204/week
$210/week
Two short visits for meals, errands, laundry, or check-ins
15 hours/week
$510/week
$525/week
Several mornings or afternoons of personal care and homemaker help
30 hours/week
$1,020/week
$1,050/week
Part-time daily support, often when ADL needs are becoming regular
56 hours/week
$1,904/week
$1,960/week
Eight hours a day, seven days a week; still not 24-hour care
These simple estimates are not quotes. They do not include possible holiday premiums, live-in arrangements, care management fees, supplies, transportation charges, or a higher rate for nursing. They do show why “just a few hours” needs to become an actual schedule before anyone can judge affordability.
A family paying RN-level rates for routine meal preparation is misallocating money. A family paying a companion to handle clinical medication problems is misallocating risk. Cost only makes sense after the care level is named correctly.
The painful surprise is that the care many families want first — help with bathing, meals, housekeeping, transportation, and supervision — is often custodial care. It may be essential. It may keep a parent out of crisis. But it is not automatically paid by Medicare.
Private Pay
Private pay means the parent or family pays directly from income, savings, retirement funds, or family contributions. This is the most flexible route because it can pay for the exact schedule the family chooses, including companionship, homemaker help, and personal care. It is also the route where hours must be watched closely because small schedule changes become large monthly changes.
Medicare
Medicare may cover home health services when the person meets Medicare’s requirements, including needing part-time or intermittent skilled services and being homebound. Medicare.gov states that covered home health services can include part-time or intermittent skilled nursing care, therapy services, medical social services, and part-time or intermittent home health aide care, but not homemaker services, meals delivered to the home, 24-hour-a-day home care, or personal care when that is the only care needed.[4]
That last phrase is the one families should underline. If the only need is help with bathing and dressing, Medicare is usually not the payer. If skilled care is needed after an illness or injury, Medicare may be relevant. Because coverage rules can change and individual circumstances matter, families should verify current rules with Medicare, the home health agency, and a State Health Insurance Assistance Program counselor before relying on coverage.
Medicaid Home- and Community-Based Services waivers may help eligible older adults receive personal care, homemaker support, respite, adult day services, or other community-based supports instead of institutional care. Eligibility, waiting lists, covered services, and consumer-directed options vary by state. This is a program to investigate early, not after the family has already exhausted savings.
VA Aid and Attendance
Veterans and surviving spouses may be eligible for VA Aid and Attendance if they meet service, financial, and care-need requirements. The benefit can help pay for assistance with daily activities. Families should check eligibility through the VA or an accredited veterans benefits representative rather than assuming military service alone qualifies someone.
Long-Term Care Insurance
Long-term care insurance may cover home care, but policies differ sharply. Look for the benefit trigger, elimination period, daily or monthly maximum, covered provider types, documentation requirements, inflation protection, and whether informal caregivers can be paid. Do this before hiring if possible, because some policies require agency licensing or care plans that a private arrangement may not satisfy.
State, Local, and Community Programs
Area Agencies on Aging, local aging departments, nonprofit programs, and community organizations may offer homemaker services, transportation, meals, respite, caregiver education, or referrals. These programs rarely solve every hour of need, but they can reduce pressure around the edges.
Tax Deductions
Some home care expenses may be relevant to medical expense deductions or dependent care tax rules, depending on who paid, why the care was needed, and whether IRS requirements are met. Keep invoices, care plans, and proof of payment, then ask a qualified tax professional. Do not build the care budget around a tax benefit until someone has checked the actual situation.
Agency or Private Hire
An agency is not automatically better, and a private caregiver is not automatically risky. The difference is who handles screening, scheduling, supervision, backup coverage, payroll, taxes, insurance, training, and complaints.
Option
What families often gain
What families must watch
Home care agency
Screening, scheduling, backup caregivers, supervision, payroll handling, liability structure, and care coordination
Higher hourly rates, minimum shifts, less control over which aide is assigned, and variable quality between agencies
Private caregiver
Potentially lower cost, more direct control, and a consistent relationship if the match is good
Employer responsibilities, taxes, backup coverage, background checks, training verification, supervision, and liability
NCOA recommends a step-by-step hiring process that includes identifying needs, deciding what type of caregiver is appropriate, seeking referrals, interviewing candidates, checking references, and setting expectations in writing.[9] That advice applies whether the family uses an agency or hires privately; the difference is how much of the work the family must do itself.
Start with credible referral points, then interview as if the details matter because they do. The federal Eldercare Locator can connect families with local aging resources. Area Agencies on Aging can explain local programs and referrals. Medicare Care Compare is relevant when comparing Medicare-certified home health agencies, not when shopping only for private-pay companion care.
Ask whether the provider offers nonmedical home care, Medicare-certified home health care, hospice, or more than one line of service.
Ask which caregiver credential will be assigned for bathing, transfers, medication reminders, dementia supervision, wound-related concerns, or post-hospital monitoring.
Ask how the care plan is created, how often it is updated, and who families call when needs change.
Ask about background checks, training, supervision, backup coverage, minimum shifts, weekend rates, and cancellation policies.
Ask what happens if the aide reports bruising, confusion, missed medications, spoiled food, unsafe transfers, or a possible decline.
Green lights are specific answers: a clear assessment process, written care plan, named supervisor, transparent rates, backup staffing plan, and a willingness to say when a nurse or home health agency is more appropriate. Red flags are vague promises, pressure to sign quickly, no written service agreement, unclear worker qualifications, reluctance to discuss supervision, or language that makes Medicare sound like a general payer for daily custodial care.
You do not need to become an eldercare expert before calling an agency. You do need enough vocabulary to keep the first conversation from drifting into the wrong category.
Write down the parent’s ADL needs: bathing, dressing, toileting, transferring, eating, walking, and grooming.
Write down the IADL needs: meals, shopping, transportation, laundry, housekeeping, medication reminders, money management, phone use, and appointments.
Separate custodial needs from skilled needs. Custodial care helps with daily living; skilled care involves nursing, therapy, or clinical services.
Estimate weekly hours before asking about price. Multiply the schedule by current hourly rates in your area, then check minimum shifts and weekend charges.
Match the payer to the service. Do not assume Medicare pays for daily personal care; check Medicaid waiver eligibility, VA benefits, long-term care insurance, local programs, and possible tax treatment.
Call providers with task-based language: “help with showers and transfers three mornings a week” is more useful than “we need a nurse.”
A good first call sounds concrete: “My mother lives alone. She can walk with a walker but needs help showering, changing clothes, preparing lunch, and getting to two appointments a month. She has no wound care or injections. We are trying to price 12 to 15 hours a week and want to know whether a PCA, CNA, or HHA is the right fit.”
That kind of call gives the provider something real to answer. It also protects the family from paying for the wrong level of care, expecting the wrong payer to step in, or missing the moment when a parent’s needs have crossed from ordinary help at home into skilled care.

Comments
Join the discussion with an anonymous comment.