Live-In Caregiver vs. 12-Hour Shifts: A Cost-and-Care Decision Framework for Families
Choosing between a live-in caregiver and rotating 12-hour shifts is a care-need match, not just a cost comparison. This guide helps adult children evaluate clinical red flags, the DOL sleep-period rule, caregiver consistency, and total costs to select the right model for their parent's situation.
By Editorial Team
live-in caregiver
24-hour home care
caregiver cost
sundowning
night wandering
care coordination
📄
A printable version of this guide is available. Use your browser's print function (Ctrl+P / ⌘P) to save or print.
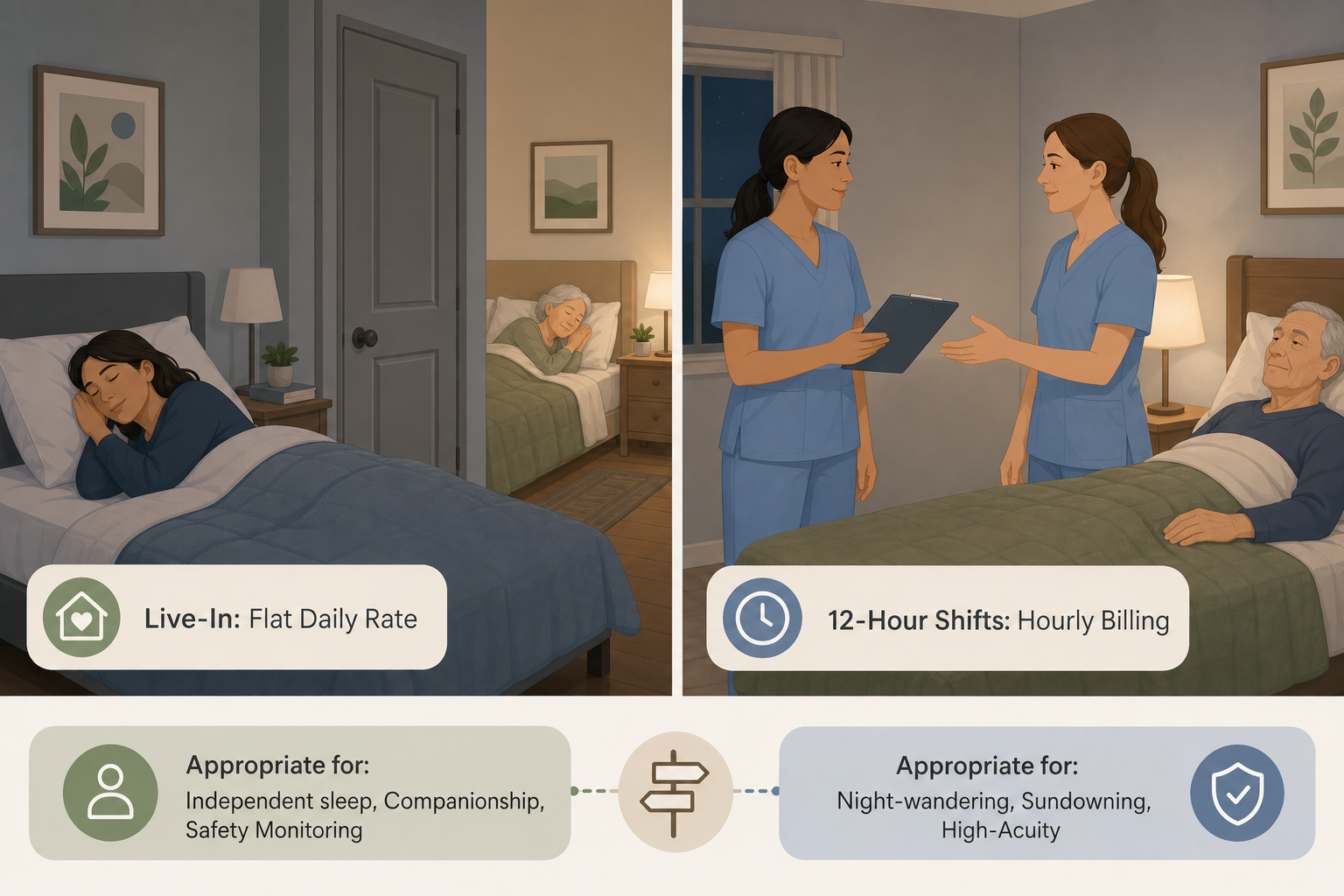
The two care models serve fundamentally different nighttime care profiles.
The Core Problem: Two Models That Look Similar but Serve Different Care Profiles
If you have already read our pricing breakdown on how much a live-in caregiver costs in 2026, you know the baseline numbers: a flat daily rate versus an hourly rate. But knowing the price is only half the equation. The harder question is which model actually works for your parent’s specific situation.
Live-in care and rotating 12-hour shifts both provide 24-hour coverage, but they are not interchangeable. The live-in model depends on a single caregiver staying in the home for multiple consecutive days, with a mandated sleep period overnight. The shift model uses multiple caregivers working staggered 12-hour shifts, meaning someone is always awake and on duty. The decision between them is not primarily a cost calculation—it is a clinical care-need match.
The central question every family must answer is this: Does the care recipient sleep through the night without significant interruptions? If the answer is yes, live-in care is likely appropriate and more affordable. If the answer is no—because of sundowning, night wandering, frequent bathroom needs, or bedbound status—then live-in care becomes unsafe, and rotating 12-hour shifts become clinically necessary, regardless of the higher cost.
Cost Comparison: Live-In vs. 12-Hour Shifts vs. 24/7 Shift Care
The table below uses Michigan market data from a nurse-led home care agency as a primary example. The national median hourly rate for nonmedical in-home care in 2026 is $34 per hour, according to A Place for Mom’s 2026 Costs of Long-Term Care and Senior Living Report, with state medians ranging from $25 per hour in Mississippi to $44 per hour in South Dakota. Your local rates will vary, but the proportional relationship between the models remains consistent.
Cost comparison of three 24-hour care models using Michigan market data from Care Plan Inc. and national median rates from A Place for Mom’s 2026 report.
Care Model
Daily Rate Range (Michigan Example)
How It Works
Key Feature
Live-In (Flat Daily Rate)
$450 – $650 per day
One caregiver stays in the home for 4–5 consecutive days; includes a mandated 8-hour sleep period with at least 5 uninterrupted hours.
Single primary caregiver; lower total cost; caregiver sleeps overnight.
12-Hour Shift (Hourly Rate)
$384 – $480 per day per shift
One caregiver works a 12-hour day shift; a second caregiver works a 12-hour night shift. Each shift is billed hourly.
Two caregivers per 24-hour period; someone is always awake; higher total cost.
24/7 Shift Care (Two 12-Hour Shifts)
$768 – $960+ per day
Two caregivers covering all 24 hours via two 12-hour shifts. This is the sum of two 12-hour shifts.
Full awake coverage; highest total cost; appropriate for high-acuity needs.
The live-in model is typically 30% to 40% less expensive than hiring hourly caregivers to cover three 8-hour shifts, according to Care Plan Inc. When compared to two 12-hour shifts, the savings are even more pronounced because the live-in flat rate covers the caregiver’s sleep time at no additional cost. However, those savings are only realized if the care recipient’s condition allows the caregiver to actually sleep.
The Live-In ‘Sleep Period’ Rule: What the DOL Requires
Many families assume that a live-in caregiver is available 24 hours a day, every hour of the day. That is not how the model works legally. Under U.S. Department of Labor guidelines, a true live-in arrangement requires the caregiver to receive a private room and a minimum of 8 hours of sleep per night, at least 5 of which must be uninterrupted. This is not a suggestion or a best practice—it is a legal requirement that defines the model.
What this means in practice: if your parent wakes and needs assistance during the caregiver’s sleep period, the caregiver is legally entitled to count that time as work and may be owed additional pay. If the interruptions are frequent enough that the caregiver cannot get 5 consecutive hours of rest, the arrangement no longer qualifies as live-in care under DOL rules. At that point, the family must shift to a shift-based model, even if the live-in daily rate seemed more affordable on paper.
Clinical Red Flags That Disqualify Live-In Care
Certain nighttime behaviors make live-in care unsafe or legally unworkable. When these conditions are present, rotating 12-hour shifts become clinically necessary, regardless of the cost difference. The National Institute on Aging identifies sundowning—increased confusion, agitation, and restlessness in the late afternoon and evening—as a common symptom in dementia that often disrupts sleep and requires active supervision.
The following clinical red flags indicate that a live-in model is likely inappropriate:
Sundowning or night agitation. If the senior becomes confused, anxious, or restless after dark and requires redirection or reassurance, the caregiver cannot reliably get 5 uninterrupted hours of sleep.
Night wandering. Wandering during the night is a safety risk that requires active monitoring. A sleeping caregiver cannot prevent a fall or a nighttime exit.
Frequent bathroom assistance (more than 2–3 times per night). Each trip to the bathroom interrupts the caregiver’s sleep period. If interruptions are frequent, the DOL sleep rule is violated.
Bedbound status requiring repositioning. Turning and repositioning a bedbound senior every 2 hours to prevent pressure injuries requires a caregiver who is awake and on duty throughout the night.
End-of-life care. Active dying often involves irregular breathing, pain, and agitation that require round-the-clock attention. Shift-based care is standard in hospice and end-of-life settings.
If any of these conditions describe your parent’s current situation, the decision is straightforward: live-in care is not a safe option. The additional cost of 12-hour shifts is not an upsell—it is the cost of adequate, safe care.
Match your parent’s nighttime behavior to the appropriate care model.
Caregiver Consistency: One Primary Person vs. a Team of Workers
Beyond cost and clinical appropriateness, the two models create fundamentally different relational dynamics. The live-in model typically assigns one primary caregiver who stays in the home for 4 to 5 consecutive days at a time. That single caregiver becomes deeply familiar with the senior’s routines, preferences, and subtle changes in condition. For seniors with early-to-mid dementia, this consistency can reduce anxiety and confusion because the same face appears each morning.
The shift model, by contrast, requires a minimum of 3 to 4 different workers per week to cover two 12-hour shifts, seven days a week. Each worker is fresher and more alert during their shift because they have had time off, but the senior must adapt to multiple caregivers with different communication styles and approaches. For some seniors—particularly those with dementia—this rotation can be disorienting.
Relational and operational trade-offs between the live-in and shift models.
Dimension
Live-In Model
12-Hour Shift Model
Number of caregivers per week
1 primary caregiver (4–5 days)
3–4 workers
Caregiver alertness overnight
Caregiver sleeps (legally required)
Caregiver is awake and on duty
Consistency for the senior
High: same person, same routines
Lower: multiple personalities and styles
Caregiver fatigue risk
Moderate: long consecutive days
Lower: shifts are shorter with rest days
Best for
Seniors who sleep through the night; early-to-mid dementia; companionship-focused care
Seniors with nighttime needs; high-acuity medical needs; sundowning or wandering
There is no universally superior model here. The live-in model offers relational depth at the cost of caregiver fatigue. The shift model offers alertness and coverage at the cost of consistency. The right choice depends on which factor matters more for your parent’s specific condition.
One primary caregiver versus a rotating team: the consistency trade-off.
Decision Matrix: Matching Care Needs to the Right Model
The table below maps common senior care profiles to the recommended care model. Use it as a starting point, then discuss the specific situation with a home care agency or geriatric care manager.
Decision matrix matching senior profiles to the appropriate care model.
Senior Profile
Nighttime Behavior
Recommended Model
Rationale
Independent sleep, high fall risk
Sleeps through the night but needs supervision during the day
Live-In
Caregiver can sleep; available for daytime safety monitoring and companionship.
Early-to-mid dementia, calm nights
Sleeps through the night; occasional confusion during the day
Live-In
Consistency of one caregiver reduces confusion; caregiver can rest overnight.
Sundowning or night agitation
Restless, confused, or agitated after dark; may call out or try to get up
12-Hour Shifts
An awake caregiver is needed to redirect and ensure safety during the night.
Night wandering
Gets out of bed and walks during the night; may try to leave the home
12-Hour Shifts
Active monitoring required; a sleeping caregiver cannot prevent wandering.
Frequent bathroom assistance (3+ times/night)
Needs help transferring to and from the bathroom multiple times per night
12-Hour Shifts
Interruptions violate the DOL sleep rule; an awake caregiver is needed.
Bedbound, requires repositioning
Cannot turn in bed; needs repositioning every 2 hours
12-Hour Shifts or 24/7 Shift Care
Round-the-clock awake care is required to prevent pressure injuries.
End-of-life / hospice
Irregular breathing, pain, agitation; may need medication management overnight
12-Hour Shifts or 24/7 Shift Care
Continuous awake care is standard in end-of-life settings.
When Families Shift Models Over the Course of a Disease Progression
Care needs are not static. A family may start with live-in care during the early stages of dementia, when the senior sleeps through the night and benefits from the consistency of a single caregiver. As the disease progresses and sundowning or night wandering emerges, the same family may need to transition to 12-hour shifts. Later, if the senior becomes bedbound or enters end-of-life care, 24/7 shift care may become necessary.
This progression is normal, and planning for it in advance can reduce stress and financial surprises. Here is a typical sequence:
Stage 1: Live-in care. Appropriate for early-to-mid dementia, independent sleep, and companionship-focused care. Cost: $450–$650/day.
Stage 2: Transition to 12-hour shifts. Triggered by the onset of sundowning, night wandering, or frequent nighttime bathroom needs. Cost: $768–$960+/day for two 12-hour shifts.
Stage 3: Consider 24/7 shift care or facility-based care. When the senior becomes bedbound, requires repositioning, or enters end-of-life care, 24/7 shift care may be needed. At this point, families should also evaluate whether a skilled nursing facility or hospice facility offers a more appropriate level of care. See our guide on when 24-hour home care costs less than a nursing home for that comparison.
The key is to monitor for the clinical red flags described earlier and to have a contingency plan in place before a crisis forces a rushed decision. If you are also weighing the broader question of whether your parent can safely age in place after a fall or functional decline, our guide on aging in place vs. assisted living after a fall can help you evaluate that next step.



Comments
Join the discussion with an anonymous comment.