Preventing Falls in Seniors with Orthostatic Hypotension: Evidence-Based Home Strategies for Caregivers
Reviewed: 2026-07-05
Preventing Falls in Seniors with Orthostatic Hypotension: Evidence-Based Home Strategies for Caregivers
This guide explains how family caregivers can reduce fall risk in seniors with orthostatic hypotension through actionable non-pharmacologic strategies — from the '3-phase' positioning technique and bolus water drinking to compression garments and home safety modifications — based on current clinical evidence.
By Editorial Team
new caregiver
experienced caregiver
long-distance caregiving
spousal caregiver
working caregiver
daily routines
medication management
personal hygiene
care coordination
first steps
ADLs
IADLs
The frightening part is usually not the diagnosis. It is the few seconds after a parent stands up: one hand reaches for the dresser, the knees soften, the face goes blank for a moment, and everyone in the room waits to see whether this is just dizziness or the beginning of a fall.
Orthostatic hypotension fall prevention for seniors starts there, in the transition. A caregiver cannot safely diagnose the cause of a blood pressure drop at the bedside, and should not try to medically manage it alone. But the home routine can be changed today so standing becomes slower, supported, hydrated, and predictable instead of rushed and improvised.
Orthostatic hypotension means blood pressure falls when a person moves upright. It is common in later life: about 20% of community-dwelling adults age 60 and older are affected, and estimates rise as high as 50% in nursing home settings.[1][2] It also matters for falls. In a 2021 study in JAMDA, orthostatic hypotension measured 30 seconds or 3 minutes after standing was associated with a significantly greater risk of falling within 12 months.[3]
New, severe, or worsening symptoms need medical evaluation, especially fainting, chest pain, shortness of breath, new neurologic symptoms, repeated near-falls, or dizziness that begins after a medication change. Some cases are neurogenic, related to autonomic nervous system failure, and can be complicated by supine hypertension; in neurogenic orthostatic hypotension, supine hypertension may occur in about 50% of cases.[1] Still, non-pharmacologic strategies are recommended as first-line management before medications because they are usually low risk and practical to begin while the medical review is underway.[1]
Start With the Moments That Usually Cause the Fall
Orthostatic hypotension does not spread its risk evenly across the day. It tends to show up when the body is asked to change position or blood flow quickly: getting out of bed, standing from the toilet, stepping out of a warm shower, rising after a meal, or walking away from a chair before the blood pressure has caught up.
Caregivers often wait for the older adult to say, “I’m dizzy.” That helps when it happens, but it is not enough. Many older adults have hypotensive unawareness, meaning the blood pressure drop may not feel dramatic to them. Watch for the behavior instead: pausing mid-stand, gripping furniture, widening the stance, sitting back down abruptly, looking suddenly tired, or saying they “just need a second.” Those are not just quirks of movement. They are useful warning signs.
Home strategy
Why it ranks high
Best use
Slow, supported position changes
Directly addresses the highest-risk transition: lying or sitting to standing
Every morning, bathroom trip, and chair rise
Pre-standing muscle activation
Uses leg and arm muscle contractions to help move blood back toward the heart
Before standing fully, especially from bed, toilet, or dining chair
Hydration and timed water bolus
Supported by physiologic rationale and expert guidance; 500 ml can raise blood pressure within 20-40 minutes in some patients[2]
Before predictable standing-heavy periods, if fluid intake is medically appropriate
Meal adjustment
Targets postprandial hypotension after larger or high-carbohydrate meals[1]
Breakfast and lunch routines, when activity often follows eating
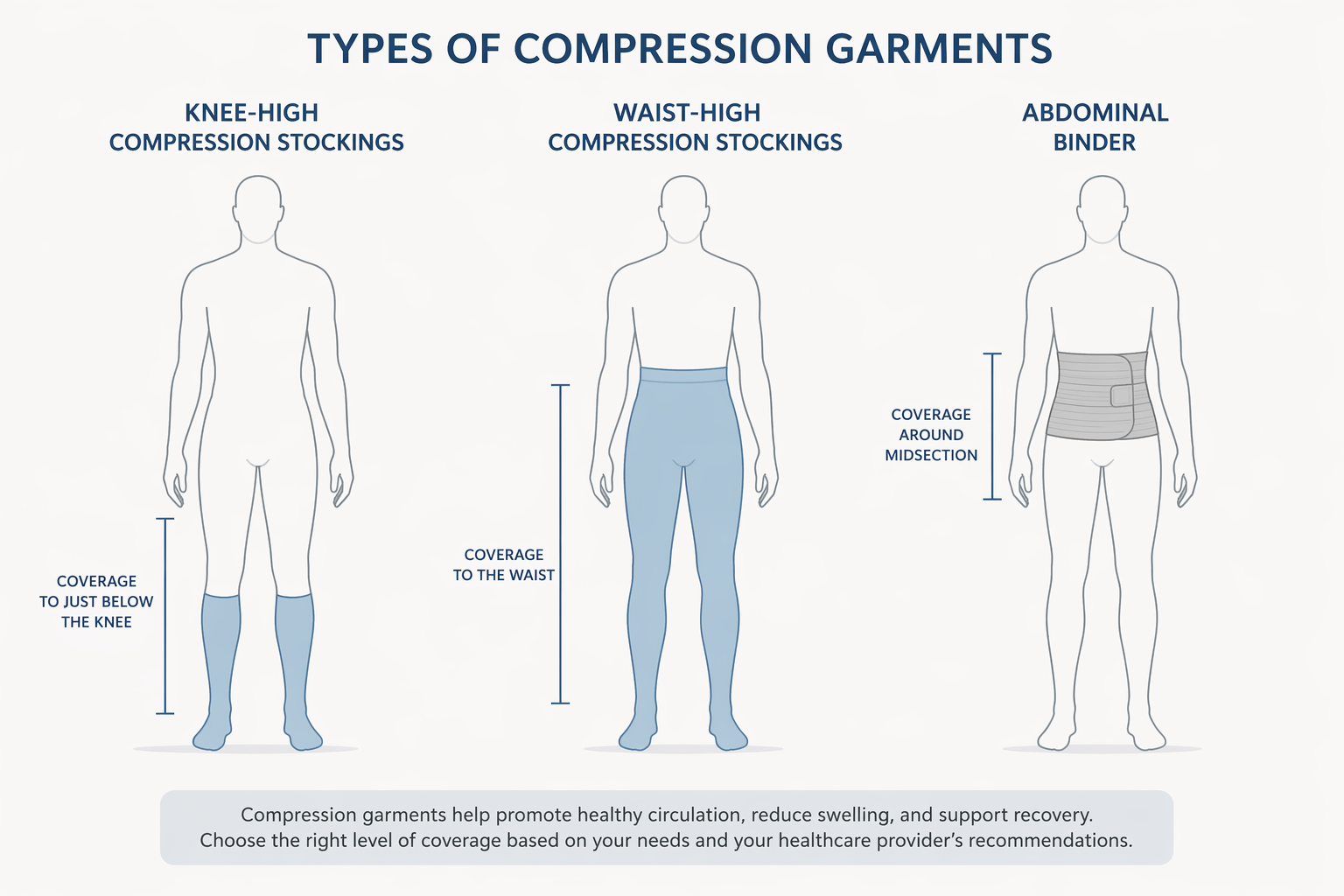
Compression garments or abdominal binder
Waist-high compression and abdominal binders address blood pooling more effectively than knee-high stockings[2]
When symptoms persist and the older adult can tolerate the garment
Medication review
Several drug classes are associated with orthostatic hypotension; changes require clinician direction[1]
After new symptoms, dose changes, or repeated near-falls
The Standing Routine: Make It Specific Enough to Repeat
“Stand up slowly” is too vague for a sleepy person at 7:15 a.m. It does not say where the feet go, what the hands hold, how long to pause, or when to sit back down. A safer instruction is concrete enough that both the caregiver and the older adult can rehearse it the same way every time.
Use a 3-phase position change
For getting out of bed, use a lying-to-sitting-to-standing sequence. The middle phase is the part families most often skip.
Lying: Before sitting up, have the older adult take a few normal breaths and move the ankles or feet if they are awake enough to follow directions.
Sitting: Help them sit at the bed edge for 1-2 minutes, with both feet flat on the floor and at least one hand on the mattress, bed rail, or a stable support.
Standing: Have them stand with support already under the hand, then pause again before walking away from the bed.
That sitting pause is not wasted time. It gives the body a chance to respond before the person adds walking, turning, slippers, conversation, and urgency. If the older adult becomes pale, unusually quiet, more unsteady, or says the room is moving, the next step is not encouragement. It is sitting back down.
Add 30 seconds of muscle activation before full standing
Before standing fully, use simple muscle contractions for about 30 seconds: pump the feet, squeeze the hands, tighten the thighs, or march lightly in place while still supported. Counter-pressure maneuvers such as leg crossing, squatting, and arm tensing are recommended in clinical guidance and tend to work best when the person has warning symptoms before the blood pressure drops fully.[1][2]
For many seniors, squatting is not a safe first choice. Start with the version that can be done without losing balance: hand squeezing while seated, foot pumps at the bed edge, or thigh tightening before rising from a chair. If the person uses a walker, the hands should not leave the walker for a maneuver once standing.
Put the support where the standing happens
Orthostatic hypotension calls for support at transition points, not just a generally tidy house. The support needs to be reachable before the person stands, not after they are already swaying.
Bed: place a stable bedside rail, transfer pole, or heavy, non-rolling support where the person’s hand naturally lands during the sitting pause.
Toilet: install properly anchored grab bars; towel bars and sink edges are not designed to take body weight.
Favorite chair: choose a firm chair with arms and enough seat height that standing does not require a deep forward lurch.
Dining area: keep the first walking path after meals clear, because post-meal blood pressure drops can overlap with standing.
This is narrower than a full home safety redesign. Broader lighting, flooring, clutter, and room-layout changes still matter, and they belong in a larger plan such as Maintaining Mobility at Home: How to Adapt Your Senior’s Living Space for Independence and Fall Prevention. For orthostatic hypotension, though, the first question is more specific: where does this person stand up, and what can they hold before the blood pressure drop shows itself?
Morning: Treat the First Upright Minutes as High Risk
Morning is often when families discover whether the plan is usable. The older adult may be groggy, need the bathroom, want privacy, or dislike being watched. A workable routine protects the transition without turning the bedroom into a nurses’ station.
Keep the first clothing step seated. Put the robe, socks, shoes, and glasses within reach of the bed or a sturdy bedside chair. Dressing while standing on one leg is risky even without orthostatic hypotension; with a pressure drop, it adds a balance challenge at the worst possible time.
Head-of-bed elevation may also help some patients. Clinical guidance describes elevating the head of the bed 30-45 degrees at night to reduce morning hypotension by limiting overnight pressure diuresis.[1] This is different from simply adding pillows under the head, which can bend the neck without raising the torso effectively. Families should ask the clinician whether this fits the person’s heart, breathing, reflux, and comfort needs.
Bathroom Transitions Need Their Own Rules
The bathroom combines several fall triggers: urgency, standing from a low toilet, warm water, wet flooring, and privacy. It is also where families often rely on the least reliable supports. A towel bar may feel sturdy until the day it is asked to hold most of a person’s weight.
Use anchored grab bars beside the toilet and in the shower or tub area.
Consider a raised toilet seat or toilet safety frame if the person has to rock forward hard to stand.
Avoid very hot showers and baths, because heat can dilate blood vessels and worsen lightheadedness.
Have the person sit to dry off, dress, and rest after bathing before walking to another room.
Keep a call button, phone, or agreed signal available if privacy is important but supervision is still needed.
If symptoms often happen after toileting or bathing, do not treat that as a general “bad balance” problem only. Bring that pattern to the clinician. Timing helps separate orthostatic symptoms from weakness, vertigo, medication effects, dehydration, and other causes.
Hydration Helps, but It Has to Be Planned
Hydration advice often fails because it arrives as a scolding: “Drink more water.” For a caregiver, the useful version is measurable and tied to the part of the day when standing is predictable.
Clinical guidance commonly gives a total fluid target of 2-2.5 liters per day for orthostatic hypotension management, when medically appropriate.[1] That target is not right for everyone. People with heart failure, kidney disease, fluid restrictions, or certain medication plans need individualized instructions.
Bolus water drinking is more specific. Drinking 500 ml, or about 2 cups, of water within 2-3 minutes can activate the osmopressor reflex and raise blood pressure within about 20-40 minutes in some people.[2] The evidence is not the same as a guarantee against falls, and it should not be presented that way. Its value at home is that it is concrete: if the clinician says fluids are safe, a caregiver can time water before a shower, therapy session, or morning routine rather than hoping casual sipping will be enough.
Ask the clinician whether a daily fluid goal is appropriate for this person.
If approved, place water where the person already pauses: bedside table, breakfast chair, and favorite daytime seat.
Use timed water before predictable upright activity, not right before rushing to the bathroom.
Track whether more fluid increases nighttime bathroom trips, because that can create a different fall risk.
Meals Can Make Standing Worse
Some falls happen after breakfast or lunch, not because the person ate “wrong,” but because blood pressure can drop after meals. Clinical guidance for orthostatic hypotension includes smaller, more frequent meals and limiting high-carbohydrate meals to reduce postprandial hypotension.[1]
At home, that may mean not scheduling the most standing-heavy task immediately after a large breakfast. If the older adult usually showers, dresses, and walks to the mailbox after eating, move one of those tasks earlier or build in a seated pause after the meal.
Sodium is the part that needs the strongest guardrail. Some clinical guidance describes increasing sodium intake in a wide range, about 2-10 grams per day, for selected patients with orthostatic hypotension.[1] That does not mean families should start salting food aggressively. Anyone with hypertension, heart failure, kidney disease, swelling, or a history of stroke or cardiovascular disease needs the prescribing clinician’s approval before changing sodium intake.
Compression: Knee-High Stockings Are Usually Not the Main Tool
Compression sounds simple until the box arrives. Many families buy knee-high stockings because they are easier to find and less intrusive. For orthostatic hypotension, that may not address enough of the blood pooling. Guidance describes waist-high compression stockings at 30-40 mmHg as more effective than knee-high stockings, and abdominal binders may be even more effective for splanchnic blood pooling.[2]
The practical question is tolerance. A garment that works physiologically but cannot be put on at home, causes skin injury, or triggers a daily argument will not become a routine. Check skin, comfort, breathing, toileting access, and hand strength. If the older adult has fragile skin, wounds, circulation problems, or significant swelling, ask the clinician before starting compression.
Option
What to know
Knee-high stockings
Often easier to apply, but generally less useful for orthostatic hypotension than higher compression coverage
Waist-high stockings
Better target for lower-body pooling; 30-40 mmHg is commonly referenced in guidance[2]
Abdominal binder
Can be especially useful when abdominal blood pooling is a major contributor; may be easier than waist-high stockings for some people[2]
When Symptoms Start, the Goal Is to Stop the Next Step
The most important caregiver response to lightheadedness is not to hurry the person to a chair across the room. It is to stop the next upright demand. If they are seated, they stay seated. If they have just stood, they hold support and sit back down if needed. If they are walking, guide them to the nearest safe seated position without turning the moment into a rushed rescue.
Counter-pressure maneuvers are most useful when warning symptoms appear early enough. Leg crossing, arm tensing, and squatting are included in orthostatic hypotension guidance, but the safest version depends on balance, strength, and cognition.[1][2] A physical therapist can help train these movements and build progressive postural conditioning, especially when the older adult has already had near-falls or is afraid to stand.
Call for urgent medical help if dizziness comes with fainting, injury, chest pain, severe shortness of breath, stroke-like symptoms, a new irregular heartbeat sensation, or confusion that does not quickly clear. Orthostatic hypotension may be common, but those signs should not be managed as a home routine problem.
Medication Review Belongs With the Clinician, Not the Pillbox
Medication lists are often where caregivers find a plausible explanation and a dangerous temptation. Several medication classes can contribute to orthostatic hypotension, including antihypertensives such as alpha-blockers and diuretics, antidepressants, antipsychotics, dopaminergic drugs used in Parkinson’s disease, opioids, and anticholinergics.[1] A retrospective study cited in clinical guidance found a 23% increased prevalence of orthostatic hypotension in older adults taking any one of these medication types.[1]
Do not stop, skip, split, or move doses without the prescriber. A blood pressure medication may be part of the problem, but the simple story that blood pressure treatment always worsens orthostatic hypotension is not accurate. In SPRINT, intensive blood pressure treatment was associated with a reduced risk of orthostatic hypotension, although most participants with orthostatic hypotension were asymptomatic.[1] The safer caregiver task is to document the pattern.
Write down when dizziness, wobbling, or near-falls happen: after waking, after meals, after bathing, after medication, or after exertion.
Bring the full medication list, including over-the-counter sleep aids, bladder medicines, pain medicines, and supplements.
Ask whether home blood pressure checks should include lying, sitting, and standing measurements, and exactly how long to wait before each reading.
Ask whether symptoms suggest neurogenic orthostatic hypotension, dehydration, medication effect, deconditioning, or another cause.
A One-Week Home Plan That Does Not Try to Fix Everything at Once
The first week should not become a stack of new rules no one can remember. Start with the transitions most likely to cause a fall, then add the strategies that fit the person’s medical situation and tolerance.
Day 1: Put the 3-phase standing routine into the morning and bathroom routine: lie, sit 1-2 minutes with feet planted, stand with support, pause before walking.
Day 2: Add 30 seconds of seated foot pumps, hand squeezes, or thigh tightening before standing from bed, toilet, and the main chair.
Day 3: Move supports to the actual transition points: bed, toilet, shower, favorite chair, and dining chair.
Day 4: If fluids are medically safe, organize the daily fluid plan and ask whether timed 500 ml water boluses are appropriate before predictable upright activity.
Day 5: Adjust meal timing and size if symptoms appear after eating; avoid placing showers, long walks, or errands immediately after a large or high-carbohydrate meal.
Day 6: Discuss sodium, compression garments, and head-of-bed elevation with the clinician if symptoms continue.
Day 7: Review the pattern log and request medication review or physical therapy referral if there are repeated symptoms, near-falls, or fear of standing.
For screening and clinical follow-up, many clinicians use fall-risk tools such as CDC STEADI resources to structure assessment and prevention planning.[4] That framework does not replace orthostatic hypotension-specific routines at home; it helps connect them to gait, strength, vision, footwear, medications, and prior fall history.
Caregivers cannot diagnose the cause of every blood pressure drop, and they should not adjust medications or sodium on their own. They can, however, make the dangerous seconds less dangerous: sit before standing, activate muscles before walking, put a real support under the hand, time fluids when appropriate, avoid heat and rushed post-meal activity, and bring a clear pattern to the clinician.

Comments
Join the discussion with an anonymous comment.