How an ADL Checklist Can Help Your Family Talk About Your Parent’s Needs
For: adult childStage: early independence15 minutesReviewed: 2026-07-05
How an ADL Checklist Can Help Your Family Talk About Your Parent’s Needs
Learn how documenting specific daily tasks with a simple checklist can turn tense family conversations into shared-evidence discussions, helping you get everyone on the same page with less denial and more action.
By Editorial Team
new caregiver
experienced caregiver
long-distance caregiving
spousal caregiver
working caregiver
daily routines
medication management
personal hygiene
care coordination
first steps
ADLs
IADLs
The conversation usually starts badly because everyone thinks they are talking about the same parent.
One adult child says, “Mom isn’t managing well.” A sibling who stopped by for lunch says, “She seemed fine to me.” The parent hears an accusation and gets defensive. The person who has been checking the refrigerator, sorting the mail, noticing the same clothes, and finding pills left in the organizer starts listing examples too quickly. Within minutes, the issue is no longer food safety, medication confusion, or unpaid bills. It is tone. It is drama. It is whether someone is “overreacting.”
An ADL checklist for an elderly parent can change that conversation, but not because a checklist magically decides what your parent needs. It helps because it gives the family a common record of what has actually happened: the task, the date or pattern, and the practical consequence. That is very different from walking into a room with a verdict.
Caregivers already go looking for answers. Family Caregiver Alliance has reported that 84% of caregivers with internet access research health topics online, a useful reminder that many families are trying to make sense of changes before they have a clear plan or a shared vocabulary.[1] The missing piece is often not concern. It is a format that other people can believe and act on.
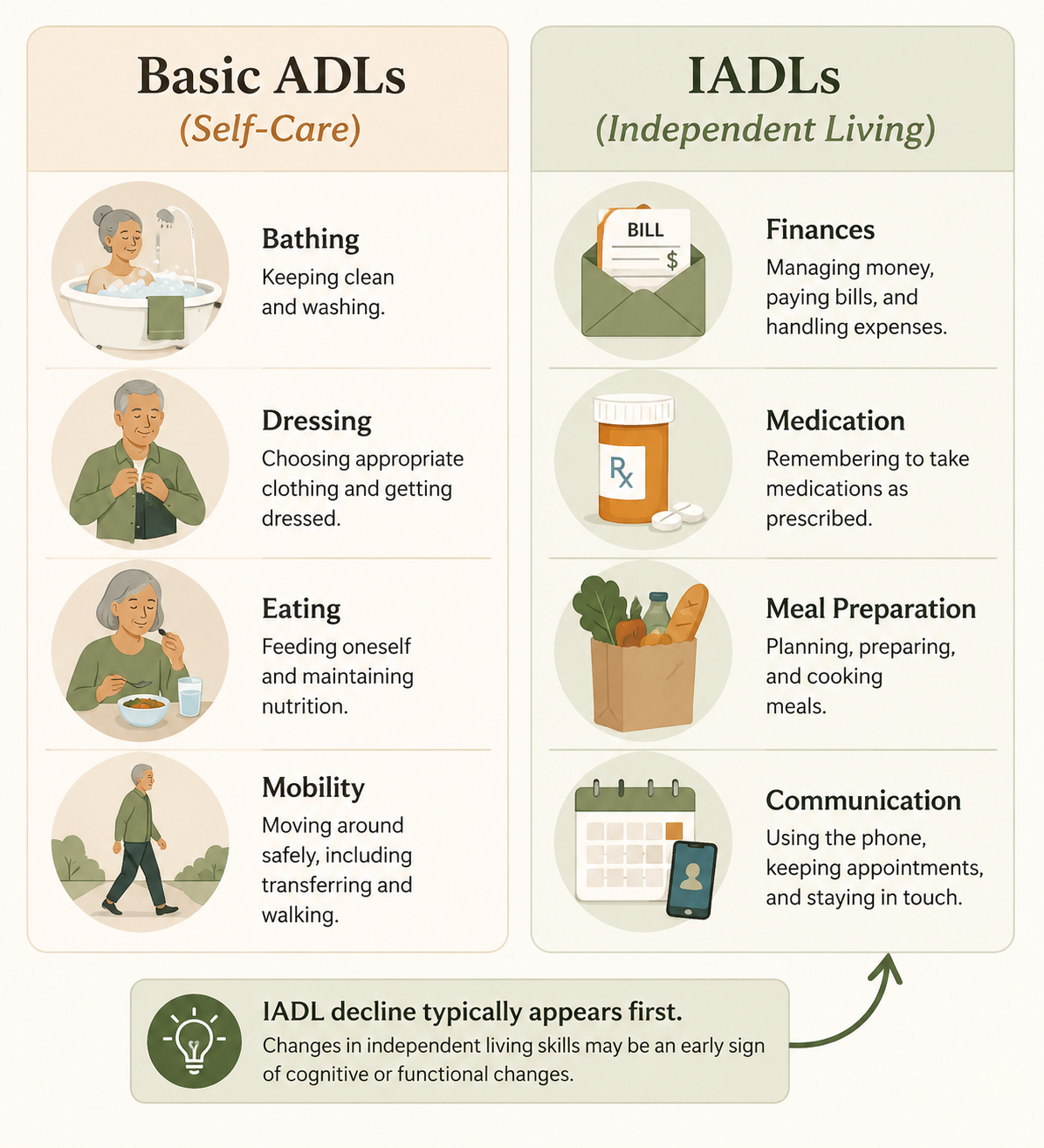
What ADLs and IADLs Actually Tell You
Activities of daily living, or ADLs, are basic self-care tasks such as bathing, dressing, toileting, transferring, continence, and eating. Instrumental activities of daily living, or IADLs, are more complex tasks that support independent living, including managing medications, preparing meals, handling money, using transportation, shopping, housekeeping, and communication.[2][3]
That distinction matters because families often wait for the more visible losses. A parent who cannot bathe safely or get to the toilet in time is hard to dismiss. But many families live for months, sometimes years, in the murkier stage: spoiled food, missed payments, confusing pill bottles, a car with new dents, or a parent who says they are eating well but has mostly crackers and expired milk in the kitchen. StatPearls notes that IADL decline can precede basic ADL decline by months or even years, and that the Lawton IADL Scale is especially sensitive to early cognitive decline.[2]
This is why “small” observations are not petty. They are often the first functional evidence that independent living is becoming harder. They still do not prove a diagnosis. They do not prove that your parent must move, stop driving, or accept a certain type of care. They simply deserve to be recorded carefully instead of argued about from memory.
Use the Checklist to Record Function, Not to Build a Case
A useful checklist is not a prosecution file. It should not make your parent sound like a collection of failures. The goal is to describe the situation clearly enough that siblings, clinicians, and your parent can see the same pattern without having to accept your emotional interpretation first.
Start with the categories clinicians already recognize, then write in ordinary language. Healthcare providers use ADL assessments in care coordination and discharge planning, which means organized observations from home can help connect a short office visit to what is happening during the rest of the week.[3]
Area to Watch
Examples to Notice
What to Avoid Writing
Bathing and hygiene
Bathing less often, body odor, trouble getting in or out of the shower, wearing visibly soiled clothing
“Dad is giving up”
Dressing
Same outfit for several days, clothing not suited to weather, difficulty with buttons or shoes
“Mom looks terrible”
Eating and meals
Expired food, weight changes you can observe, skipped meals, trouble using the stove safely
“She can’t feed herself anymore” unless you observed that directly
Mobility and transfers
Difficulty rising from a chair, holding walls while walking, near-falls, avoiding stairs
“He is going to fall any day”
Medication management
Pills left in organizer, duplicate doses, confusion about timing, expired prescriptions still in use
Missed appointments, getting lost, trouble arranging rides, not returning important calls
“She should never go anywhere alone” as a first note
If you need a deeper task-by-task breakdown, use an IADL assessment guide alongside your notes. For this conversation, though, the categories are only the starting point. The real work is how you document what you see.
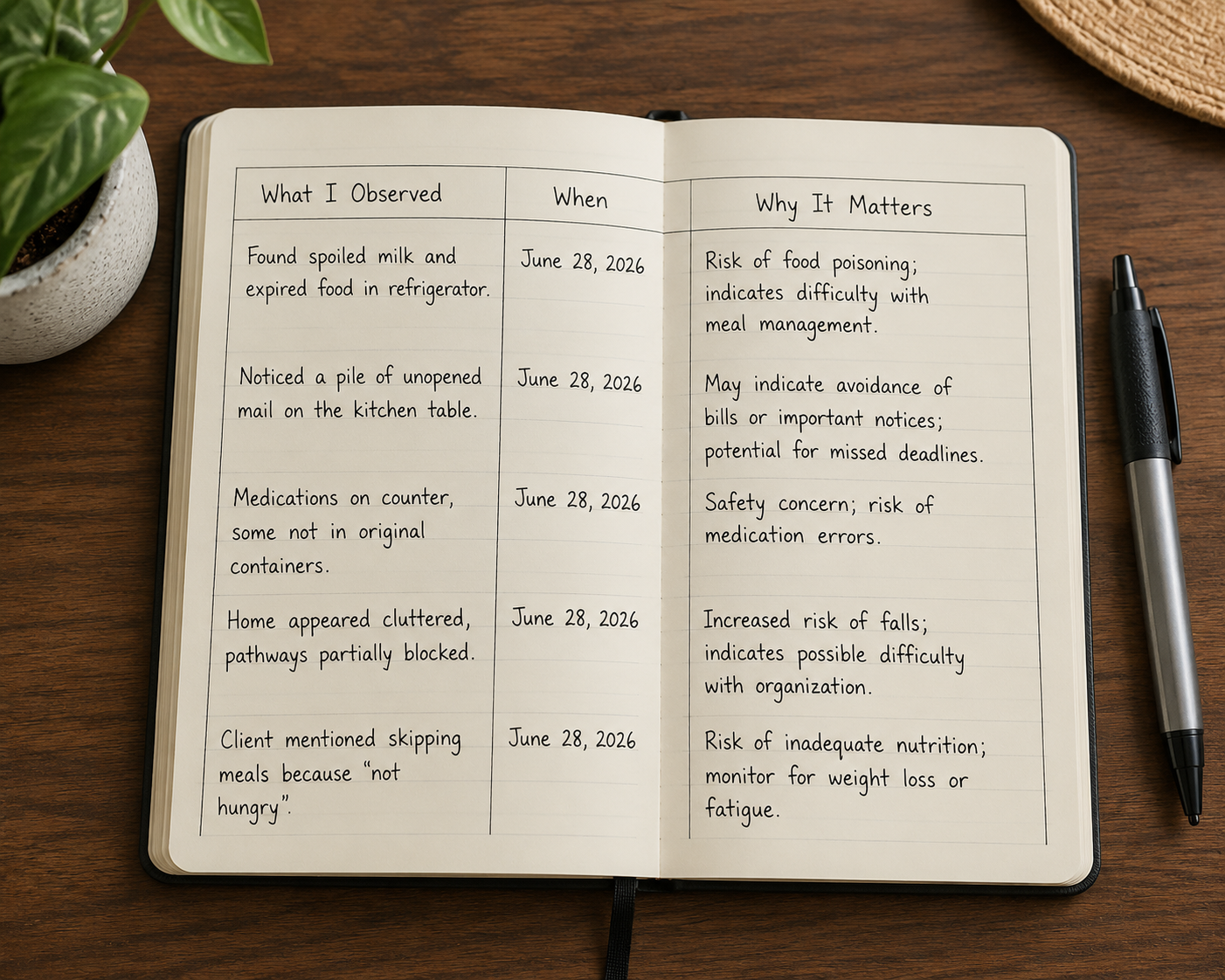
The Three-Column Method: What, When, Why It Matters
The most useful ADL checklist is simple enough to keep using. Three columns are enough: what you observed, when you observed it, and why it matters. The third column is important because it connects the observation to safety, health, independence, or decision-making without turning the note into an insult.
What I Observed
When
Why It Matters
Found spoiled milk and several expired prepared meals in the refrigerator.
Saturday visit; similar expired food noticed two weeks earlier.
May mean meal planning, shopping, or food safety is becoming difficult.
Medication organizer still had pills in Monday and Tuesday slots when I visited Friday.
Friday afternoon.
Could mean doses were missed or the organizer is confusing.
Electric bill had a past-due notice in the unopened mail pile.
First noticed June 18; another notice found July 2.
May indicate bill management is slipping and utilities could be affected.
Parent wore the same visibly stained shirt during three visits.
Three visits over about ten days.
Could signal trouble with laundry, bathing, dressing, memory, or energy.
Parent held the wall from bedroom to bathroom and paused twice before sitting.
Sunday morning.
May affect fall risk and toileting safety, especially at night.
Notice what these entries do not say. They do not say “unsafe,” “stubborn,” “dementia,” “lazy,” or “can’t live alone.” Those may be the fears running underneath the observation, but they are not the observation itself.
Column 1: Write What Happened, Not What You Think It Means
A clean observation can be checked by someone else. “There were three unopened past-due notices on the kitchen counter” is stronger than “Dad is bad with money now.” “The pill organizer had four missed doses” is stronger than “Mom can’t manage medication.” The first version gives a sibling or clinician something to ask about. The second version invites an argument about your attitude.
When you are not sure what happened, say that. “I could not tell whether the pills were missed or the organizer had been refilled incorrectly” is still useful. It tells the doctor or family that medication management needs review without pretending you know the cause.
Column 2: Capture Dates, Frequency, and Patterns
One missed bill may be ordinary. Three notices in six weeks are different. One skipped shower after an illness may not mean much. A month of avoiding bathing because the tub feels frightening means the family needs to solve a specific problem.
If exact dates feel too formal, use a consistent pattern: “week of July 6,” “last three Sunday visits,” or “twice this month.” The point is not courtroom precision. The point is to stop every conversation from depending on who remembers what under stress.
Column 3: Explain the Practical Consequence
The “why it matters” column should answer a plain question: what could happen if this continues? Spoiled food matters because of food safety. Missed pills matter because the medication plan may not be working as prescribed. Unopened mail matters because bills, insurance notices, or appointment instructions can be missed. Trouble getting out of a chair matters because toileting, bathing, and leaving the home may become harder.
Keep this column practical. “May need a medication review” is useful. “She refuses to admit she needs help” may be true in a broader emotional sense, but it does not help anyone decide the next care step.
A Simple Rating System Can Keep the Notes Consistent
You do not need a clinical scoring tool to start a family conversation. A simple three-level rating can help siblings see change without arguing over every single example.
Rating
Use It When
Example
Independent
Your parent completes the task safely and reliably without help.
Pays monthly bills on time and can explain what was paid.
Needs support
Your parent can do part of the task but needs reminders, setup, supervision, transportation, or backup.
Takes medication correctly when the organizer is filled by someone else.
Unable or unsafe without help
The task is not happening, is happening unsafely, or creates a significant risk if no one assists.
Leaves stove burners on or repeatedly misses essential medications.
Use the rating to summarize a pattern after you have examples, not to label your parent on a bad day. A parent recovering from a short illness may need temporary help. A parent who repeatedly cannot complete the same task over time needs a different kind of conversation.
How the Same Checklist Changes Three Conversations
The same notes can be used badly or well. If you wave the checklist like proof that everyone should finally admit you were right, the room will close down. If you use it to slow the conversation and name the next question, it can help people stop defending themselves long enough to look at the facts.
With Siblings: Move From Impressions to Patterns
Sibling disagreement often comes from different levels of exposure. The person who visits for holidays sees a parent who can rally for a meal. The person nearby sees the unopened mail, the laundry, the fridge, the repeated phone calls about the same appointment, and the way the parent moves when no guest is expected.
Bring the notes as a pattern, not as a complaint. Instead of “You don’t understand how bad it is,” try framing the issue around a task: “I want us to look at medication and bills over the last month because I’m seeing repeated problems there.” That keeps the conversation closer to what needs solving.
Share the three-column notes before asking for a major decision.
Separate observed facts from possible explanations.
Ask siblings to add their own observations using the same format.
Assign one next step, such as scheduling a medication review or checking whether bills are current.
If the bigger family conversation includes driving, finances, memory, or moving, this checklist works well as pre-work before a broader hard conversation with aging parents. It gives everyone something more solid than “I just have a bad feeling.”
With Your Parent: Make It You and Them Against the Problem
A parent who hears “I made a checklist about what you can’t do” will probably defend themselves. Most of us would. The gentler and more honest approach is to name the task that has become harder and look for support around that task.
For example: “I noticed the medication organizer has been hard to keep straight. I don’t want you to have to worry about whether a dose was missed. Can we ask the pharmacist or doctor to review the setup?” That is different from “You can’t handle your pills.” The first version protects dignity and still takes the risk seriously.
When resistance is high, keep the first ask smaller than the whole fear. You may be worried about whether your parent can keep living alone. The first practical question may be whether someone can review medications, install a shower grab bar, arrange grocery delivery, or sit down together with the bills. If every observation turns into the largest possible conclusion, your parent has to fight the conclusion before they can even hear the observation.
For situations where the answer to every offer is no, pair your notes with a communication and boundary-setting guide for a parent who refuses help. Documentation does not remove the emotional difficulty, but it can keep you from restarting the same argument from the beginning each time.
With a Clinician: Bring the Week They Do Not See
Doctors, nurse practitioners, therapists, and social workers may see your parent for a short, structured encounter. Your parent may be rested, prepared, and determined to appear fine. That does not mean the clinician is careless. It means an office visit is a snapshot.
Your notes bring the rest of the week into the room. Instead of saying, “I think something is wrong,” you can say, “In the past month, I found missed medication doses twice, two past-due notices, and spoiled food during three visits. What should we evaluate first?” That gives the clinician a way to ask follow-up questions, consider medication management, screen for cognitive or physical changes, or refer to therapy or care coordination when appropriate.
This is also where restraint matters. Do not ask the checklist to do work it cannot do. It does not diagnose dementia, prove incapacity, or establish benefits eligibility by itself. Medicaid and other program rules vary by state, and care-level decisions depend on more than one family checklist. What your notes can do is make the right questions harder to avoid.
How to Answer the Objections Without Escalating the Fight
You do not need a perfect speech. You need a way to return to the documented pattern without humiliating your parent or attacking your sibling. These are not lines to memorize; they are the shape of a calmer response.
Objection
What It Usually Means
How the Checklist Helps
“I’m fine.”
Your parent may hear the concern as a threat to independence.
Return to one task and one pattern: medication, meals, bills, bathing, or transportation. Ask for help solving that task rather than demanding a global admission.
“You’re overreacting.”
A sibling may have seen fewer examples or may be afraid of what the examples imply.
Show dates and repeated observations. Invite them to add their own notes using the same rating system.
“The doctor didn’t say anything.”
The family may be treating a short visit as proof that nothing is changing.
Explain that clinicians see a limited snapshot and bring the home pattern to the next appointment.
“This is just aging.”
The family may be minimizing because the alternative feels overwhelming.
Separate normal aging from specific functional consequences: missed doses, unsafe cooking, unpaid bills, falls, or skipped hygiene.
The aim is not to win the exchange. It is to keep the conversation attached to observable function long enough for the family to choose a responsible next step.
What to Document for Two to Four Weeks
If there is no immediate emergency, gather observations for a defined period. Two to four weeks is often enough to reveal whether you are seeing isolated incidents or a pattern. If safety is urgent, do not wait to complete a checklist before calling a clinician, emergency service, or local support agency.
Meals and food safety: expired food, weight-related concerns you can observe, skipped meals, unsafe stove use.
Medication management: missed doses, duplicate doses, confusion about purpose or timing, trouble refilling prescriptions.
Money and mail: unpaid notices, unopened important mail, unusual purchases, difficulty understanding bills.
Hygiene and dressing: bathing changes, soiled clothing, same outfit repeatedly, trouble with fasteners or laundry.
Mobility and home safety: near-falls, furniture-walking, trouble with stairs, difficulty rising from chairs or getting in and out of bed.
Transportation and appointments: missed appointments, getting lost, unsafe driving concerns, inability to arrange rides.
If your observations are already pointing toward safety concerns at home, a guide to warning signs your parent can no longer live alone can help you sort which risks need faster action. Use that kind of guide to sharpen your questions, not to jump over the conversation your family still needs to have.
When the Checklist Shows a Real Change
Once the notes show a pattern, the next step is not always a dramatic one. Sometimes the answer is a medication review, a home safety evaluation, grocery support, bill-pay assistance, transportation help, or a follow-up appointment. Sometimes the notes raise harder questions about memory, mobility, driving, or whether the current living setup still works.
Bring the notes to the next family conversation or medical appointment and ask the narrowest useful question: “What support would reduce this risk?” “What should be evaluated?” “Who can take responsibility for this task for the next month?” “What would tell us that the current plan is no longer enough?”
If you are still in the early stage of noticing that something is off, a recognition guide for adult children can help you name the broader pattern. If the checklist has already made the need clearer, move into a practical action plan for helping elderly parents so the family can divide responsibilities instead of circling the same debate.
An ADL checklist helps because it slows everyone down. It gives the person who has been noticing the evidence a fair way to present it. It gives siblings a way to verify and participate. It gives your parent a better chance of being treated with dignity while real risks are addressed. Start with what happened, when it happened, and why it matters. Then use those notes to decide the next question that actually needs answering.

Comments
Join the discussion with an anonymous comment.