What Aging in Place Modifications Actually Cost and Save
Reviewed: 2026-07-09
What Aging in Place Modifications Actually Cost and Save
This article breaks down the real costs of home modifications for aging in place and the evidence on what families save — helping you decide whether to invest in the home or budget for assisted living.
By Editorial Team
new caregiver
experienced caregiver
long-distance caregiving
spousal caregiver
working caregiver
daily routines
medication management
personal hygiene
care coordination
first steps
ADLs
IADLs
After a fall, the family math gets very real very fast. Someone is holding the discharge papers. Someone is asking whether the bathroom is safe. Someone else, usually from farther away, is asking whether it makes sense to spend money on a house if assisted living may be coming anyway.
That is the right question, but it is often asked too late and too broadly. Aging in place modifications do not have to mean a whole-house remodel. The more useful question is narrower: what level of modification is enough to reduce real risk now, and how does that compare with the cost of another fall, more paid help, or a move to care?
The strongest cost-benefit evidence is surprisingly modest. A Washington University/Somerville program serving older adults in St. Louis found that a community-based home modification intervention reduced falls by 38%. The average cost was $765 per person, while estimated healthcare savings were $1,613 per person, roughly a 2:1 return from avoided medical costs alone.[1]
That number matters because it is not an elevator sales pitch. It is closer to the kind of work families actually put off: grab bars, safer steps, better lighting, a shower that does not require a balance test every morning. The finding does not prove that every home project pays for itself, and it does not tell you what a contractor will charge in your zip code. It does show that small, targeted changes can be financially serious.
The 2:1 ROI Evidence Is Useful Because It Is Limited
The Washington University/Somerville program is the right place to start, and also the wrong place to stop. It ran in one city, St. Louis, from 2015 to 2017.[1] Local labor costs, housing stock, participant health, and program design all affect whether another community would see the same return.
Still, the scale of the finding changes the family conversation. A $765 intervention is not competing with a $50,000 remodel. It is competing with the next emergency room visit, the next round of physical therapy, the next frantic call from a neighbor, and the possibility that one preventable fall accelerates a move no one has budgeted for.
The study also measures healthcare savings, not every family cost. It does not count the adult child missing work, the spouse who stops sleeping well, or the paid aide added because everyone is afraid of the shower. Those costs are harder to put into a clean spreadsheet, but they are often the costs that finally force a decision.
So the practical conclusion is not “modify everything.” It is that waiting for certainty can be more expensive than making a small, evidence-informed first move.
Most Useful Changes Are Not Luxury Remodels
Families often hear “aging in place modifications” and picture a gutted bathroom, a residential elevator, and a contractor’s estimate that makes assisted living look simple. Those projects exist. They are not where most families need to begin.
Cost tier
Typical projects
What the spending is really buying
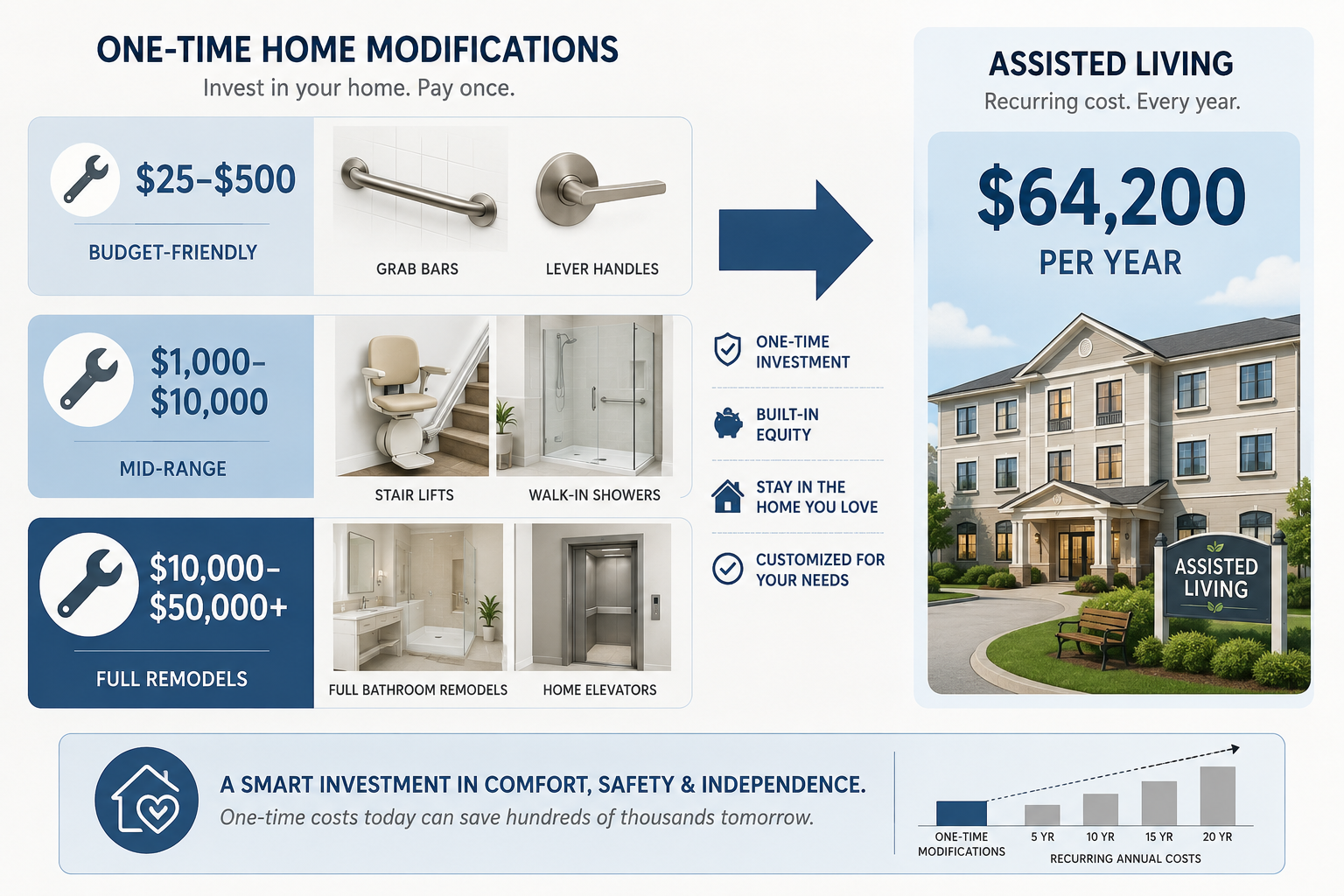
$25–$500
Grab bars, lever handles, motion-sensor lighting, non-slip surfaces
Fewer balance challenges in the places where falls often become care crises
Access to key rooms without relying on a spouse, adult child, or aide every time
$10,000–$50,000+
Full bathroom remodels, major layout changes, elevators
Longer-term accessibility when the home itself blocks safe daily living
Industry pricing guides place many basic aging-in-place changes in the $25 to $500 range, including grab bars, lever-style door handles, and motion-sensor lighting.[2] These are not glamorous upgrades. They are the difference between a parent using the bathroom alone and someone needing to hover nearby just in case.
The mid-range is where the decisions get harder, because the dollar amounts start to feel like “real” money. The National Council on Aging places stair lifts at about $2,500 to $8,000.[3] Other 2026 accessibility pricing guidance puts walk-in showers around $6,000 to $12,000, with larger projects such as full remodels or elevators moving into the $10,000 to $50,000-plus range.[4]
A stair lift should not be treated as the same kind of decision as a grab bar. A full bathroom rebuild should not be treated as the same kind of decision as better lighting. Lumping all of it together is how families talk themselves out of doing anything.
A better first pass is to separate the work by what failure it prevents. A grab bar prevents a specific loss of balance. A ramp preserves entry and exit. A stair lift may preserve access to the bedroom or shower. A full remodel only makes sense when smaller changes cannot solve the actual daily obstacle.
Why the Small-Cost Data Should Calm the Room
The best national cost-distribution data is old, but still useful because it shows what kinds of spending older adults actually reported. An ASPE/HHS analysis using a 2006 Health and Retirement Study module found that 40% of older adults who added home modifications paid less than $100 out of pocket.[5]
That does not mean today’s prices are the same. They are not. It also does not mean families can solve every serious mobility problem for under $100. The value of the finding is simpler: “home modification” includes a lot of small, practical changes, not only contractor-led renovations.
If your parent’s home has no secure place to hold near the shower, no light on the route to the bathroom, loose rugs, and round doorknobs that are hard to turn with arthritis, the first budget conversation should not begin with a full remodel. It should begin with the hazards that can be removed this week.
The Assisted Living Comparison Is Annual, Not One-Time
The comparison that often gets missed is timing. Many home modifications are one-time expenses. Assisted living is recurring. Choice Mutual reports an average assisted living cost of $64,200 per year, while also noting broader aging-in-place statistics such as more than 1 in 4 older adults falling each year and only 18% of adults 50 and older having made home changes.[6]
That $64,200 figure should not be treated as your family’s quote. Assisted living costs vary sharply by region, apartment type, and level of care. Memory care, medication management, bathing assistance, and transfer help can change the bill. A low-cost region and a high-cost metro area are not the same budget problem.
But even with that caution, the direction of the math is important. A $2,500 stair lift is not financially equivalent to moving. A $10,000 bathroom project is painful, but it may still be less than a few months of assisted living. A $25,000 package of entry, bathroom, and stair changes deserves scrutiny, but it should be compared against the annual cost of care, not against a vague feeling that “the house should be fine.”
The harder question is whether the modification actually delays or prevents the need for paid care. Sometimes it does. Sometimes the parent’s dementia, medical complexity, or need for hands-on help makes the house only one part of the decision. The home can remove barriers; it cannot provide supervision by itself.
A Practical Phasing Plan
The cleanest way to keep the family from freezing is to phase the work. Not everything has to be done now. Not everything should wait.
Phase
Decision standard
Examples
Do now
Low cost, obvious hazard, no major downside
Grab bars, lighting, rug removal, hand-held showerhead, lever handles
Price and plan
A daily activity is becoming unsafe or dependent on another person
The project changes structure, plumbing, layout, or long-term care feasibility
Major bathroom remodel, bedroom relocation, elevator, whole-home accessibility plan
The “do now” phase is where families often save the most stress for the least money. If the hospital discharge notes mention fall risk, or your parent is already furniture-walking through the hallway, waiting for a perfect long-term plan is not discipline. It is exposure.
The “price and plan” phase needs more care. A stair lift, ramp, or shower conversion should match the parent’s actual routine. If the only full bathroom is upstairs, the stair decision affects bathing, not just convenience. If there are two steps at the front door and no safe rail, the entry decision affects every appointment, grocery trip, and emergency exit.
Room-by-room prioritizing helps here because the family should not spend evenly across the house. Bathrooms, stairs, entries, and nighttime routes usually deserve attention before cosmetic improvements. A detailed room-by-room aging in place remodel priority guide can help turn a contractor walk-through into a sequence instead of a wish list.
The professional-input phase is where a Certified Aging in Place Specialist, occupational therapist, or accessibility contractor may be worth the fee. If a project affects structure, plumbing, stairs, transfers, or the parent’s ability to remain home for more than a few months, the family should not rely only on a hardware-store guess. A guide to when to hire a Certified Aging in Place Specialist is most useful once the obvious low-cost fixes are already identified.
Homeowners Have More Options Than Renters
The financial case for modification is strongest when the family can actually modify the home. That is where the equity gap becomes hard to ignore. The ASPE/HHS analysis found that homeowners were 4.74 times more likely than renters to add modifications.[5]
That gap is not just preference. Owners can approve work, borrow against equity, and decide that a bathroom change is an investment in continued use of the property. Renters may need landlord permission, may not want to pay for permanent improvements, and may be limited to removable equipment.
For renters, the first round may need to emphasize portable ramps where appropriate, tension-mounted or non-permanent aids only when safe and properly rated, lighting, furniture layout, shower chairs, and landlord-approved grab bars. The return-on-investment argument may still apply, but the path to action is narrower.
Funding also belongs after the family understands the actual scope. Grants, loans, tax deductions, Medicaid waiver possibilities, veterans’ benefits, and local programs may matter, but they should not blur the first decision: which risks are immediate and what does it cost to reduce them? Once that list exists, a funding guide for aging in place home modifications becomes much more useful.
When Spending on the House Is Not the Stronger Move
There are cases where the spreadsheet points away from the house. If a parent needs round-the-clock supervision, is unsafe using appliances, cannot transfer even with equipment, or has rapidly increasing care needs, structural changes may make the home safer without making it workable.
There are also projects that are too large for the likely benefit. A $50,000 remodel for a parent who may need memory care in six months is a different decision from a $500 set of bathroom and lighting changes after a first fall. The right comparison is not “home good, facility bad.” It is whether a specific home investment buys meaningful safety, independence, or care-time reduction for long enough to justify the cost.
This is also why device-level claims deserve caution. A product can be sensible without having the same evidence base as a full community program. A grab bar installed in the right place is different from a rail that is poorly placed, ignored, or used in a way no one assessed. The practical standard is not whether a catalog says “senior safe.” It is whether the change fits the person, the task, and the room.
The Decision Families Can Defend
If siblings want a defensible plan, put the first budget in three columns: immediate low-cost fixes, priced mid-range projects, and care-cost comparison. The first column should move quickly. The second should get local quotes. The third should use real assisted living prices in the parent’s region, not national averages alone.
The Washington University/Somerville evidence gives families permission to take small modifications seriously: $765 in average program cost, 38% fewer falls, and $1,613 in estimated healthcare savings per person.[1] The cost-tier data keeps the conversation from jumping straight to the most expensive projects. The assisted living comparison reminds everyone that doing nothing is not free.
Proactive, incremental modification is often the financially stronger first move after fall risk appears. It is not a blank check for every renovation. It is a way to spend first where the house is making daily life more dangerous, more dependent, or more expensive than it needs to be.

Comments
Join the discussion with an anonymous comment.