What kind of in-home care does your aging parent need?
Use the ADL/IADL assessment to determine exactly what type of in-home care your aging parent needs — from a few hours of companionship to skilled nursing — without overreacting or underinvesting. Learn how to match specific functional deficits to the right service type, understand costs, and know when to consider facility care.
By Editorial Team
new caregiver
experienced caregiver
long-distance caregiving
spousal caregiver
working caregiver
daily routines
medication management
personal hygiene
care coordination
first steps
ADLs
IADLs
The first signs are often too small to settle anything. Unopened mail has started to pile up. Food in the refrigerator is past its date. Your mother wears the same shirt every time you stop by. Your father says he is “fine,” but the pharmacy refill history says something else. A bruise appears, and no one can explain whether it came from a fall, a bump, or forgetfulness.
That is usually the moment families jump to the wrong question: “Does my parent need in-home care?” The better question is more exact: which daily functions are no longer reliable, who is qualified to help with those functions, and how many hours would that actually take?
A family can love someone intensely and still hire for the wrong problem. Companion visits will not solve unsafe bathing. A home health nurse will not come indefinitely to cook dinner because Medicare approved a short skilled episode. A sibling who promises to “check in more” may not be able to cover medication setup, transportation, laundry, and shower safety every week without eventually becoming the weak link in the plan.
Start With Functions, Not Feelings
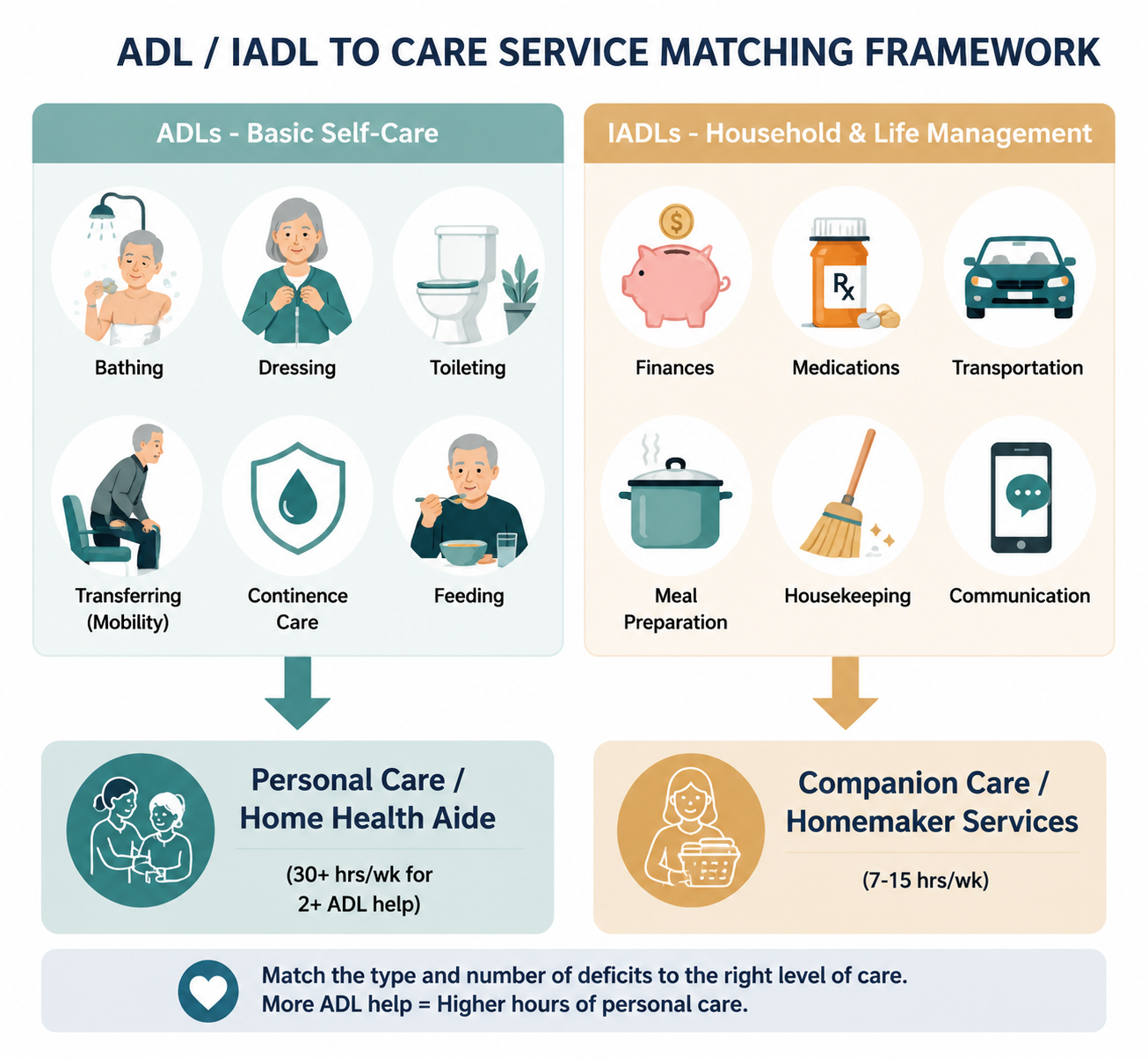
The most useful first sort is the difference between Activities of Daily Living and Instrumental Activities of Daily Living. ADLs are the basic body-level tasks: bathing, dressing, toileting, transferring, continence, and feeding. IADLs are the household and community tasks that make independent living work: managing finances, medications, transportation, meal preparation, housekeeping, and communication. Better Health While Aging describes these as standard geriatric-care categories, with the Katz Index used for ADLs and the Lawton Scale used for IADLs.[1]
That distinction matters because a parent who is still bathing, dressing, toileting, transferring, and eating safely may need a very different plan from a parent who cannot step into the shower without hands-on help. Both may be “declining.” They do not need the same service.
A simple way to begin is to write observations under two columns instead of turning them into conclusions. “Forgot to pay the electric bill” belongs under finances, an IADL. “No clean clothes” may point to housekeeping or laundry, also IADLs. “Stopped showering” may be an ADL issue, but it needs a closer look: is the problem fear of falling, pain, depression, memory, embarrassment, or lack of grab bars? The care decision starts with the task that is failing, then asks why.
If you want a more detailed worksheet for this part, use an IADL assessment guide before you call agencies. The goal is not to diagnose your parent from the kitchen table. It is to make the next professional conversation less vague.
Turn Observations Into an ADL/IADL Snapshot
Do not score your parent only on what they can do once on a good day. Score reliability. Can they bathe safely every time? Can they remember medications without a daughter calling twice a day? Can they arrange transportation to the doctor and get home with the right instructions? Can they prepare enough food over a week, not just make toast when someone is watching?
What you see
Likely function to check
Why it matters
Spoiled food, weight loss, little evidence of cooking
Meal preparation, shopping, possibly feeding
Meal preparation is an IADL; feeding is an ADL. The difference changes the service level.
Medication setup and reminders may be IADL support; clinical medication issues may need a licensed professional.
Bills unpaid, unusual donations, shutoff notices
Finances and communication
The problem may require family oversight, bill pay support, or legal/financial safeguards.
Body odor, matted hair, repeated clothing
Bathing, dressing, laundry
Laundry is an IADL; bathing and dressing are ADLs requiring more personal assistance.
New bruises, furniture walking, trouble rising from a chair
Transferring, mobility, fall risk
Hands-on transfers and fall risk may require personal care support and a medical evaluation.
This snapshot should include what family is already doing. If your brother pays the bills, your sister orders groceries, you fill the pill organizer, and a neighbor drives to church, your parent may look more independent than they really are. The assessment should name both the parent’s abilities and the invisible scaffolding around them.
ADL and IADL tools are screening tools, not verdicts. A physician, occupational therapist, physical therapist, or geriatric care manager can help evaluate cognition, home safety, mobility, medication risk, and whether a change is temporary or progressive. The family’s job at this stage is to bring usable evidence, not to pretend the form removes grief or disagreement.
Match the Deficit to the Service
Once the failing functions are named, the service menu becomes less blurry. The National Institute on Aging describes home-based supports such as personal care, homemaker services, meal help, transportation, money management help, and health-related services for older adults living at home.[2] Johns Hopkins Medicine separates home health service types by scope, including physician care, nursing care, therapy, home health aides, homemaker or basic assistance care, and companionship.[3]
Those labels are not interchangeable. They decide who can do the work, what an agency may legally assign, and what your family should expect to pay for privately.
Unsafe bathing, hands-on transfers, wound care, or medication decisions
Laundry, light housekeeping, meal preparation, grocery support
Homemaker services
Personal hygiene help if the worker is not assigned or trained for hands-on personal care
Bathing, dressing, toileting, transferring, continence support, feeding help
Personal care aide or home care aide
Skilled nursing tasks or therapy
Personal care plus support during a Medicare-covered skilled home health episode
Home health aide under a home health plan
Open-ended custodial care when there is no qualifying skilled need
Wound care, injections, monitoring after hospitalization, therapy, skilled clinical needs
Skilled home health nursing or therapy
General household help as the main purpose of care
A parent who is mostly independent in ADLs but slipping on IADLs may start with companion or homemaker help: two or three visits a week for meals, laundry, errands, mail sorting, and transportation. A parent who needs help with bathing and dressing is in a different category. Once hands-on body care is required, the plan has to cover privacy, safety, timing, and backup coverage when the aide is sick or the parent refuses help.
For a deeper comparison of service labels after you have identified the main deficit, use an elderly home care options guide or a senior care options glossary. Definitions are not paperwork trivia here; they protect you from buying companionship when the real gap is toileting help.
When IADLs Are the Main Problem
If the ADLs are intact and the IADLs are fraying, start modestly and deliberately. Seven to 15 hours a week may cover several shorter visits for meals, housekeeping, errands, appointment transportation, medication reminders, and social contact. At a $34 hourly rate, that rough range runs about $1,190 to $2,550 a month before agency minimums, weekend rates, or local price differences are added.
The work still needs a named owner. If an aide takes your parent to the grocery store but no one checks whether bills are being paid, the plan has a hole. If the aide reminds your father to take medication but no one notices that the prescription was never refilled, the reminder system is only pretending to work.
When ADLs Are Failing
Two or more ADL problems usually change the scale of care. Bathing help cannot always wait until Friday. Toileting problems do not respect a four-hour agency minimum. Transfer risk may be worst at bedtime, during the night, or first thing in the morning. This is where families often discover that the issue is not whether they care enough; it is whether the schedule is actually built around the moments of risk.
Personal care at 30 or more hours a week is a much larger commitment. Using 2026 national median private-pay figures around $34 to $35 per hour, A Place for Mom’s June 2026 cost data places in-home care in that range nationally, with monthly projections that rise quickly as weekly hours increase.[4] SeniorLiving.org’s February 2026 cost data similarly reports national home care costs in the mid-$30s per hour, while emphasizing state-by-state variation.[5]
At roughly $34 per hour, 30 hours a week is about $4,416 a month. That number is not a recommendation; it is a reality check. If your parent needs help with morning hygiene, evening toileting, meal preparation, laundry, transportation, and medication oversight, a plan built on “someone will stop by a few times” may be less expensive only because it leaves needs uncovered.
Do Not Confuse Medicare Home Health With Ongoing Custodial Care
Medicare home health coverage has rules. Medicare.gov states that covered home health services generally require that a doctor or allowed provider certify the need, that the person be homebound, and that the person need part-time or intermittent skilled services such as skilled nursing care, physical therapy, speech-language pathology, or continued occupational therapy.[6]
That is not the same as open-ended help with bathing, meals, laundry, and supervision because living alone has become hard. Medicare.gov also states that Medicare does not cover 24-hour-a-day care at home, meals delivered to the home, homemaker services unrelated to the care plan, or personal care when it is the only care needed.[6]
This distinction prevents a common and expensive family misunderstanding. A parent discharged from the hospital may qualify for skilled home health for a period of recovery. That does not mean Medicare has approved a permanent aide to handle showers, groceries, and household routines. If you need the coverage details in plain language, read the Medicare home health aide hours FAQ before building a budget around hours Medicare is unlikely to cover.
Put Costs After the Care Need, Not Before It
Costs belong in the plan, but not at the beginning. If the family starts with “What can we afford?” it may understate risk. If it starts with “Mom needs full-time care,” it may overspend before anyone has identified the actual deficits. The cleaner order is: function first, service type second, hours third, payment fourth.
Functional picture
Likely starting point
Private-pay implication at about $34/hour
ADLs intact; mild IADL strain
Companion or homemaker help, 7–15 hours/week
About $1,190–$2,550/month
ADLs intact; multiple IADLs unreliable
More structured homemaker/companion schedule plus family oversight
Cost depends on visit frequency, transportation needs, and agency minimums
Two or more ADLs need hands-on help
Personal care, often 30+ hours/week
About $4,416/month at 30 hours/week
Skilled nursing or therapy need after illness, injury, or decline
Physician-ordered home health if Medicare criteria are met
Coverage rules differ from private custodial care
Needs approach or exceed 44+ hours/week and risk remains uncovered
Reassess home care versus facility-based care
Private home care can become financially and logistically difficult
The national median is only a starting point. Local wages, agency minimums, weekend or overnight premiums, rural availability, and the level of hands-on care can change the actual quote. Before signing, ask whether the quoted rate covers transportation time, care planning, backup aides, supervisory visits, and higher-acuity personal care.
Once the likely care level is clear, a paying-for-home-help guide is the right next document. Payment planning is much more useful after the family knows whether it is pricing five hours of errands or daily body care.
Build the First Plan as a Test, Not a Family Treaty
The first care plan does not have to settle the next five years. It should cover the current deficits, assign responsibility, and set a review date. A reasonable first plan names the tasks, the worker type, the schedule, the family contact, and the conditions that would trigger a reassessment.
Task: bathing twice a week, laundry weekly, medication refill tracking, transportation to appointments.
Worker type: personal care aide for bathing and dressing; homemaker help for laundry and meals; family or professional care manager for medication oversight.
Schedule: specific days and times, with backup instructions if the aide cannot come.
Family role: one person reviews agency notes, bills, missed visits, and changes in condition.
Review trigger: fall, hospitalization, repeated missed medications, new incontinence, unsafe transfers, caregiver burnout, or refusal of essential care.
Resistance should be expected, especially around bathing, money, and strangers in the home. Precision helps here too. “We are hiring someone to help with showers on Tuesday and Friday because the tub transfer is unsafe” is usually better than “We think you need care.” It preserves what the parent can still do and names the part that is no longer safe to improvise.
Home modifications, transportation programs, meal delivery, adult day services, and fall-prevention supports may reduce the number of paid aide hours needed, depending on the situation. For the broader support ecosystem around the home, an aging-in-place services guide can help identify what belongs outside the aide schedule.
When Home Care Needs to Be Reassessed
Escalation is not proof that home care failed. It may mean the care contour changed. A parent who once needed help with meals may later need toileting help, transfer assistance, overnight supervision, dementia-related safety monitoring, or skilled wound care. The correct response is not to defend the original plan; it is to reassess the functions.
Facility care becomes a valid option when the hours, risk, and coordination burden no longer fit a safe home plan. A common threshold for reassessment is when care needs approach or exceed 44 hours a week and still leave unsafe gaps. At that point, the family is no longer comparing “home” with “not home” in a simple emotional sense. It is comparing a complex private staffing arrangement with a setting built for continuous coverage.
Advanced dementia can change the decision even sooner. Wandering, unsafe cooking, nighttime activity, aggression, or inability to summon help may require memory-care-specific planning rather than a standard companion or homemaker schedule. The ADL/IADL framework still helps describe what is failing, but it does not replace a dementia-informed evaluation.
The defensible next action is usually small and concrete: list the failed ADLs and IADLs, confirm them with a clinician or care manager when risk is significant, match each deficit to a qualified service type, price the hours honestly, and set the date when the answer will be revisited.
Comments
Join the discussion with an anonymous comment.