Which Overnight Care Option Is Right for Your Parent? A Risk-Based Decision Matrix for Falls, Wandering, Incontinence, and Sundowning
A structured guide for adult children whose parent has had a nighttime incident. Learn how to assess your parent's risk profile across four key domains and match it to the right care model — sleeping night, waking night, live-in, or respite — with side-by-side 2026 cost projections.
By Editorial Team
overnight care
fall prevention
dementia wandering
sundowning
caregiver decision-making
📄
A printable version of this guide is available. Use your browser's print function (Ctrl+P / ⌘P) to save or print.
Why Most Families Overpay for Overnight Care
The phone rings at 2:00 AM. Your parent has fallen on the way to the bathroom, or they are standing at the front door in a nightgown, confused and trying to leave. In the days that follow, fear — not data — drives the decision. The natural instinct is to hire the most intensive supervision available: a waking night caregiver who stays alert for the entire shift, or a 24/7 live-in arrangement. That instinct is understandable, but it is also expensive, and often unnecessary.
The cost gap between care models is substantial. Sleeping night care — where a caregiver rests but remains available to assist up to about twice during the night — runs approximately $200 per night nationally. Waking night care, where the caregiver stays alert for the full shift, typically costs $250 to $420 per night. Over a 30-day month, that difference can mean paying $6,000 for sleeping care versus $12,600 for waking care — a gap of more than $6,000 per month for a level of supervision your parent may not actually need.
The solution is not to guess. It is to assess your parent's actual nighttime risk profile across four specific domains — fall risk, wandering/exit-seeking, incontinence, and sundowning severity — and then match that profile to the appropriate care model. Families who do this can save 40–50% on monthly costs while still keeping their parent safe.
The Four Nighttime Risk Domains That Determine Care Needs
Not all nighttime incidents are the same. A fall caused by a rushed trip to the bathroom requires a different care response than a dementia-related wandering episode. To choose the right model, you need to understand the four risk domains that drive nighttime care needs.
1. Fall Risk (Nocturia and Mobility)
Falls are the most common nighttime emergency. According to the CDC, more than one out of four older adults falls each year, and falling once doubles the chances of falling again. The primary driver of nighttime falls is nocturia — waking up to urinate. The numbers are striking: 20–30% of all falls happen at night, and up to one in four involve a nighttime trip to the bathroom.
The risk escalates with frequency. A peer-reviewed review in the Advances in Geriatric Medicine and Research found that having two or more episodes of nocturia per night was significantly associated with recurrent falls (odds ratio 1.6, 95% CI 1.0–2.7). For context, roughly 85% of women over 65 have at least one nocturia episode, and nearly 70% have two or more. When you combine frequent nighttime urination with limited mobility — using a walker, unsteady gait, or needing to navigate a dark hallway — the fall risk becomes a nightly hazard.
2. Wandering and Exit-Seeking
Wandering at night is a hallmark of middle-stage dementia, often driven by sundowning — increased confusion, agitation, and restlessness that begins in the late afternoon and extends into the night. A person who wanders may attempt to leave the house, check doors repeatedly, or pace the hallways for hours. This behavior is not just disruptive; it is dangerous. A wandering senior can fall, become lost, or suffer exposure if they manage to get outside.
The care implication is clear: if your parent is actively exit-seeking or pacing at night, a sleeping caregiver who may not hear a quiet exit is not sufficient. As one care guide notes, exit-seeking, door checking, and sundowning-related agitation typically require awake overnight care with stronger safety planning.
3. Incontinence and Toileting Independence
Urinary incontinence is one of the most underreported risk factors for nighttime falls. Over 80% of women over age 65 have some type of urinary incontinence, according to NHANES 2015–2018 data cited in the same medical review. Urge incontinence — the sudden, uncontrollable need to urinate — is particularly dangerous. The same review found that urge incontinence doubles fall risk in older women (odds ratio 1.94, 95% CI 1.33–2.84).
The key question is not just whether your parent has incontinence, but whether they can manage it independently at night. A senior who can get to the bathroom safely, use a bedside commode, or manage incontinence products without assistance presents a lower risk than someone who needs help with toileting, changing, or cleaning up after an accident.
4. Sundowning Severity
Sundowning is not a single behavior — it is a spectrum. For some seniors, it means mild confusion and restlessness in the evening that resolves with reassurance. For others, it means hours of agitation, shouting, pacing, or aggression that requires active redirection and supervision throughout the night.
The severity of sundowning directly determines whether a sleeping caregiver model is safe. If your parent's sundowning is limited to occasional calling out or brief confusion that resolves quickly, a sleeping caregiver who can respond as needed may be sufficient. If the sundowning involves sustained agitation, attempts to leave, or aggressive behavior, a waking caregiver is likely necessary.
How to Assess Your Parent's Risk Profile: A Step-by-Step Self-Assessment
Use the following self-assessment to categorize your parent as low, moderate, or high risk in each domain. Be honest about what you observe — overestimating safety is as risky as overestimating danger.
Self-assessment guide for the four nighttime risk domains. Use this to categorize your parent's risk level in each area.
Risk Domain
Low Risk
Moderate Risk
High Risk
Fall Risk (Nocturia + Mobility)
Wakes 0–1 times per night; uses bathroom independently; no history of nighttime falls; good balance and mobility without assistive device.
Wakes 2 times per night; uses walker or cane; one nighttime fall in the past 12 months; some unsteadiness when getting out of bed.
Wakes 3+ times per night; needs assistance transferring from bed to bathroom; history of recurrent nighttime falls; uses wheelchair or requires physical support.
Wandering / Exit-Seeking
No dementia diagnosis; no history of nighttime wandering or confusion; sleeps through the night consistently.
Mild dementia; occasional confusion at night but does not attempt to leave the bed or room; responds to verbal reassurance.
Moderate to advanced dementia; active exit-seeking behavior; attempts to leave the house; paces or checks doors repeatedly; does not respond to redirection.
Incontinence / Toileting Independence
No incontinence; fully independent with toileting; can manage clothing and hygiene without help.
Occasional urge incontinence; uses incontinence products independently; can get to bathroom or bedside commode without assistance.
Frequent incontinence; needs help with toileting, changing, or cleaning up after accidents; cannot manage incontinence products alone.
Sundowning Severity
No sundowning symptoms; calm and oriented in the evening; falls asleep without difficulty.
Mild sundowning: some confusion or restlessness in the evening that resolves within 30–60 minutes with reassurance; no agitation or aggression.
Moderate to severe sundowning: sustained agitation, shouting, pacing, or aggression for 2+ hours in the evening; requires active redirection; may not respond to calming techniques.
The Decision Matrix: Matching Risk Profile to Care Model
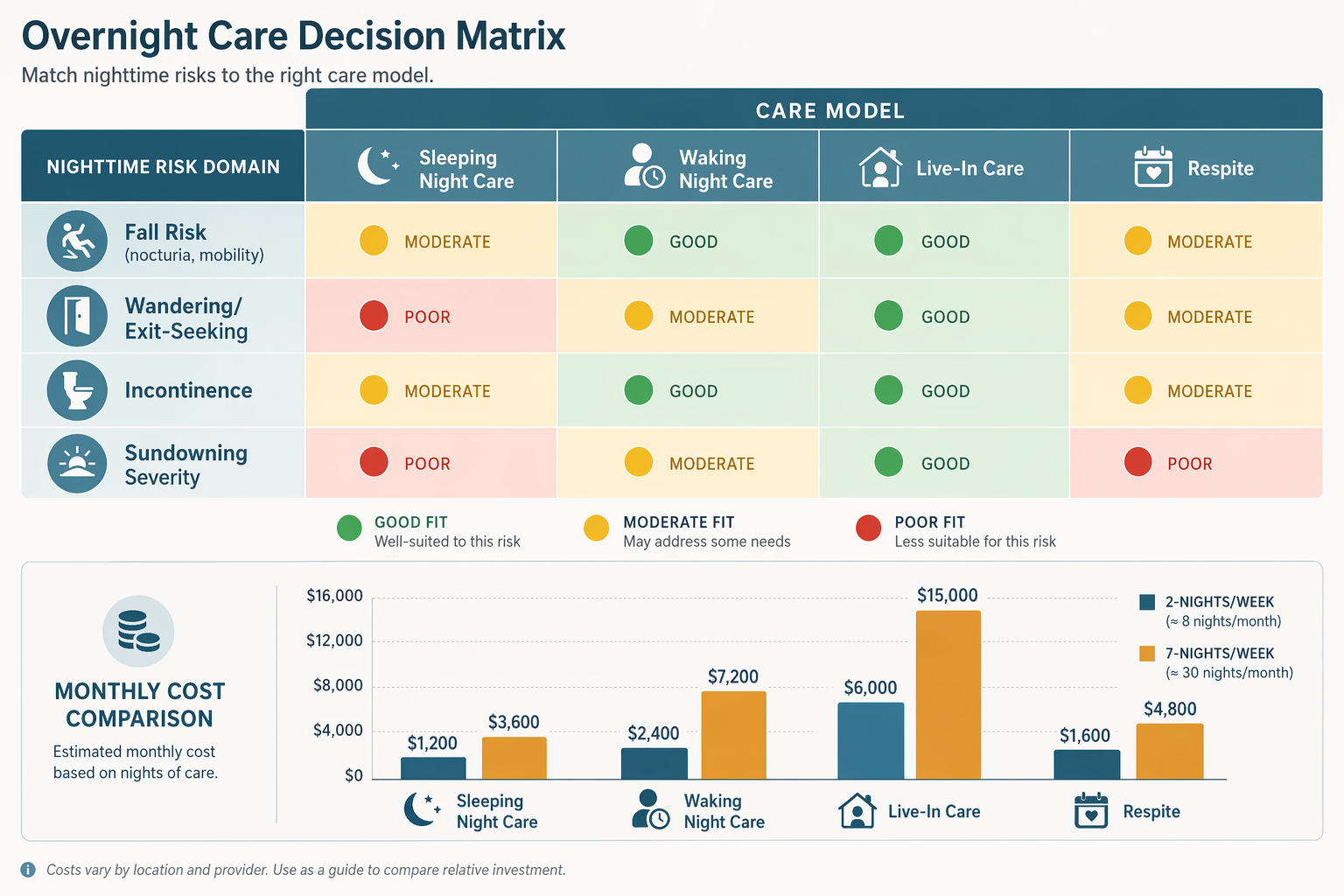
Once you have assessed your parent's risk profile, use the decision matrix below to identify which care model is the best fit. The matrix uses a traffic-light system: green means the model is a good fit for that risk level, yellow means it may work with additional precautions, and red means the model is likely insufficient.
Risk-based decision matrix for overnight care models. Green = good fit, Yellow = possible with precautions, Red = mismatch.
Decision matrix mapping risk profiles to care models. Green = good fit, Yellow = possible with precautions, Red = mismatch. Cost projections are national medians from 2025–2026 sources.
Risk Profile
Sleeping Night Care (~$200/night)
Waking Night Care ($250–$420/night)
Live-In Care ($200–$350/day)
Respite / Adult Day Care (~$115/day)
Low in all 4 domains
Green — Good fit. Caregiver rests; responds to occasional needs.
Yellow — Possible but overkill. Higher cost for minimal need.
Yellow — Possible if daytime needs are high, but not needed for nights alone.
Green — Good fit for occasional relief or planned breaks.
Moderate fall risk, low others
Yellow — May work if caregiver can assist with 1–2 transfers per night.
Green — Good fit if transfers are frequent or unsteady.
Yellow — Possible if daytime care is also needed.
Green — Good for planned respite.
High fall risk (3+ nocturia, mobility issues)
Red — Insufficient. Sleeping caregiver may not hear or respond in time.
Green — Good fit. Active monitoring for every transfer.
Yellow — Possible only if caregiver can stay awake; not a substitute for awake care.
Red — Not appropriate for active nighttime needs.
Active wandering / exit-seeking
Red — Unsafe. Sleeping caregiver may not detect a quiet exit.
Green — Good fit. Active supervision and safety planning required.
Red — Not appropriate if wandering is frequent or unsafe.
Red — Not appropriate for active nighttime wandering.
Frequent incontinence, needs toileting help
Yellow — May work if needs are predictable and limited to 1–2 episodes.
Green — Good fit for frequent or unpredictable toileting needs.
Yellow — Possible if daytime care is also needed.
Red — Not appropriate for overnight toileting needs.
Moderate to severe sundowning
Red — Insufficient. Sustained agitation requires active redirection.
Green — Good fit. Caregiver stays alert for redirection and safety.
Red — Not appropriate if sundowning involves sustained agitation.
Red — Not appropriate for evening/nighttime sundowning.
Side-by-Side Cost Comparison: Sleeping Night vs. Waking Night vs. Live-In vs. Respite
The table below shows estimated monthly costs for each care model at two common frequencies: 2 nights per week (for families who need occasional coverage) and 7 nights per week (for full-time overnight support). Costs are based on 2026 national median benchmarks.
Monthly cost comparison for overnight care models at 2 and 7 nights per week, using 2026 national median benchmarks from SeniorSite, CareYaya, A Place for Mom ($34/hour), and SeniorLiving.org ($115/day adult day care).
Care Model
Per-Night / Per-Day Cost (2026 National Median)
Monthly Cost — 2 Nights/Week
Monthly Cost — 7 Nights/Week
Best For
Sleeping Night Care
~$200/night
~$1,600
~$6,000
Seniors with low to moderate risk who need occasional assistance (1–2 wakeups per night) but not active supervision.
Waking Night Care
$250–$420/night
$2,000–$3,360
$7,500–$12,600
Seniors with high fall risk, active wandering, frequent toileting needs, or moderate to severe sundowning.
Live-In Care
$200–$350/day
$2,800–$4,900 (2 days)
$6,000–$10,500 (30 days)
Seniors who need daytime and nighttime support but have limited nighttime interruptions. Not a substitute for awake care.
Respite / Adult Day Care
~$115/day
~$920 (2 days)
~$3,450 (30 days)
Planned short-term relief for family caregivers. Not appropriate for active nighttime needs.
The potential savings from matching care intensity to risk profile are substantial. A family whose parent has low fall risk, no wandering, and mild sundowning could pay $6,000/month for sleeping night care instead of $12,600/month for waking night care — a savings of 52%. Over a year, that difference exceeds $79,000.
When to Reassess: Risk Profiles Change as Conditions Progress
A risk profile is not a one-time assessment. Dementia progresses, fall risk changes with medication adjustments, and incontinence patterns evolve. A care model that works today may be insufficient in three months.
Plan to reassess your parent's risk profile in these situations:
After any fall or near-fall — even if no injury occurred.
After a medication change, especially for blood pressure, sleep aids, diuretics, or dementia medications.
Every 3–6 months for progressive conditions like Alzheimer's or Parkinson's.
After a hospitalization or significant health event (infection, surgery, stroke).
If you notice new or worsening sundowning, wandering, or incontinence patterns.
If the primary family caregiver experiences burnout or sleep deprivation that affects their own health.
When you reassess, repeat the self-assessment from this guide and consult the decision matrix again. If your parent's risk profile has shifted from moderate to high in any domain, it may be time to move from sleeping night care to waking night care — or from live-in care to a rotating 24/7 schedule.
For a deeper look at how dementia-specific behaviors like sundowning and wandering affect overnight care decisions, see our guide on overnight care for elderly parents with dementia. For families whose risk assessment indicates they need around-the-clock support, our 24-hour home care decision guide provides next-step guidance.
Practical Next Steps and Checklist
Use this checklist to move from assessment to action. Each step builds on the one before it.
Complete the self-assessment for all four risk domains using the table above. Be honest about what you observe.
Consult the decision matrix to identify which care model(s) match your parent's risk profile.
Discuss the results with your parent's primary care provider or geriatrician. Ask specifically about fall risk, medication side effects, and whether a home safety assessment is warranted.
Interview home care agencies with the recommended model in mind. Ask whether they offer sleeping night care, waking night care, or both, and whether their caregivers are trained for dementia-specific needs.
Request itemized cost quotes from at least three agencies. Compare not just hourly or nightly rates, but also whether the agency charges extra for overnight shifts, weekends, or holidays.
Set a reassessment reminder for 3 months from now. Add it to your calendar or phone. If your parent has a progressive condition, set recurring reminders every 3–6 months.
Consider complementary safety measures that can reduce the need for awake care: motion-activated night lights, bedside commodes, bed alarms, and home modifications like grab bars in the bathroom and hallway.

Comments
Join the discussion with an anonymous comment.