Home Care vs. Assisted Living vs. Memory Care: How to Match Care to Your Loved One's Needs
By Editorial Team
home care
assisted living
memory care
ADLs
caregiver decision-making
senior care costs
Why Comparing Home Care, Assisted Living, and Memory Care Is the Most Common Decision Families Face
When a parent's health declines — after a fall, a dementia diagnosis, or a noticeable loss of function — families quickly realize that the vague term "senior care" actually refers to several distinct options, each designed for a different combination of needs. The three most frequently confused are home care, assisted living, and memory care. They are not interchangeable, and choosing incorrectly can mean moving your loved one twice, exhausting financial reserves faster than necessary, or placing them in an environment that cannot safely meet their needs.
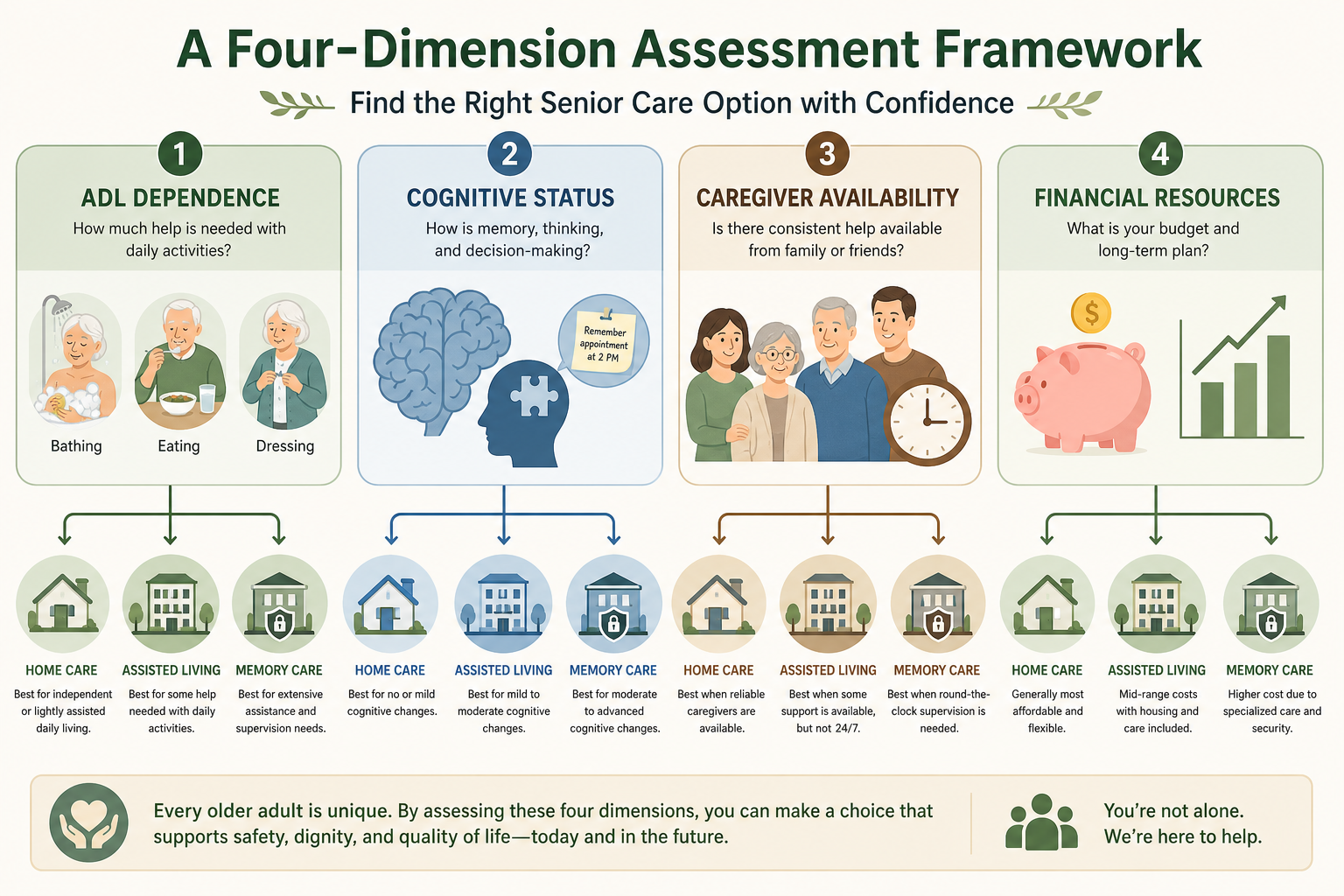
This guide provides a structured way to compare these three options using four specific assessment dimensions: ADL dependence, cognitive status, caregiver availability, and financial resources. Rather than offering a generic overview of every care type, it focuses on the decision that most families actually face: should we bring help into the home, move to a residential community, or seek a specialized dementia care environment?
The four dimensions that determine whether home care, assisted living, or memory care is the right fit.
Dimension 1: ADL Dependence — How Many Activities of Daily Living Need Support?
The number and frequency of activities of daily living (ADLs) that require assistance is the single strongest predictor of which care setting is appropriate. ADLs include bathing, dressing, eating, toileting, transferring (moving from bed to chair), and continence management. Instrumental activities of daily living (IADLs) — medication management, meal preparation, housekeeping, transportation — are also relevant but typically require less intensive support.
Here is how each care setting handles ADL dependence:
Home care: Best suited for seniors who need help with 1–3 ADLs and can manage the rest independently. A home health aide typically provides personal care (bathing, dressing, grooming) and homemaker services (meals, light housekeeping). Care is scheduled in hourly blocks, so the family must coordinate coverage for the hours the aide is not present.
Assisted living: Designed for residents who need moderate assistance with 2–4 ADLs. Staff provide scheduled help with bathing, dressing, medication reminders, and meals. Most communities use a tiered pricing model: the base rent covers a set number of ADL supports, and additional fees apply as care needs increase.
Memory care: Appropriate when ADL dependence is driven by cognitive decline — for example, forgetting to eat, dressing inappropriately for the weather, or being unable to complete a transfer safely. Memory care units provide 24/7 supervision and structured assistance with all ADLs, including toileting and continence care.
Dimension 2: Cognitive Status — Memory Loss, Wandering Risk, and Behavioral Changes
Cognitive status is the dimension that most sharply differentiates assisted living from memory care. A person with mild cognitive impairment or early-stage dementia may do well in an assisted living community that offers medication reminders and social engagement. But as the disease progresses — when wandering, sundowning, agitation, or repetitive questioning emerge — the general support model of assisted living becomes insufficient.
Key cognitive factors that determine the appropriate setting include:
Wandering risk: Memory care units are designed with secure exits, enclosed outdoor spaces, and continuous monitoring. Assisted living communities typically do not have the same level of security, and a resident who wanders may be at risk of leaving the building unnoticed.
Behavioral symptoms: Agitation, aggression, and sundowning require staff trained in de-escalation and non-pharmacological interventions. Memory care staff receive specialized training in dementia care; assisted living staff generally do not.
Safety awareness: A person who no longer recognizes safety hazards — leaving the stove on, attempting to climb a fence, or walking into traffic — needs a secured environment. Home care can provide supervision during scheduled hours but cannot offer the 24/7 containment that memory care provides.
The Alzheimer's Association notes that specialized memory care programs are available in some assisted living facilities, but the level of security and staff training varies widely. Families should ask specifically about staff-to-resident ratios, dementia-specific training requirements, and whether the unit is a locked wing within a larger community or a stand-alone facility.
Dimension 3: Caregiver Availability — Family Support, Geography, and Work Schedules
The feasibility of home care depends heavily on the availability of family caregivers. Home care agencies provide professional aides for a set number of hours per week, but the family typically fills the gaps — coordinating schedules, managing medications, handling transportation, and responding to emergencies. When the family caregiver lives nearby, is retired, or has a flexible work schedule, home care can be a sustainable option. When the primary caregiver works full-time, lives in another state, or is also elderly, the gaps become dangerous.
The financial value of unpaid family caregiving is staggering. According to the USC Schaeffer Institute, family caregivers provide an estimated $247 billion in unpaid dementia care annually. This figure reflects the economic value of care that families absorb — but it also represents a hidden cost: the wages lost, careers paused, and health impacts experienced by caregivers themselves.
Consider these caregiver availability scenarios:
Local, retired, or part-time caregiver: Home care with 20–30 hours per week of professional support may be sustainable. The family caregiver handles mornings, evenings, and weekends.
Long-distance or full-time working caregiver: Home care becomes logistically complex and expensive. The family may need 40+ hours of professional care per week, which can exceed the cost of assisted living.
Spousal caregiver who is also elderly: The physical demands of caregiving — lifting, transferring, bathing — can exceed the spouse's capacity. Facility-based care often becomes necessary for safety.
Cost is often the deciding factor, and the numbers can be counterintuitive. Many families assume home care is the cheapest option, but at 44 hours per week — roughly the amount needed to cover a workday — home care costs approximately $80,080 per year (CareScout 2025, via U.S. News). That is more expensive than the median annual cost of assisted living, which ranges from $65,028 to $75,756 depending on the source.
Memory care carries a premium of 15–25% over assisted living, with a national median of $8,019 per month (SeniorLiving.org, May 2026). This premium reflects specialized staffing, enhanced security features (cameras, secure exits, enclosed outdoor spaces), and better staff-to-resident ratios.
National median cost ranges for home care, assisted living, and memory care in 2026.
Care Option
Monthly Cost Range
Annual Cost Range
Source & Notes
Home care (44 hrs/week)
$6,677
$80,080
CareScout 2025; nonmedical caregiver at $35/hr
Assisted living
$5,419 – $6,313
$65,028 – $75,756
A Place for Mom (March 2026) vs. SeniorLiving.org (May 2026)
Memory care
$8,019 (median)
$96,228
SeniorLiving.org (May 2026); 15–25% premium over assisted living
Two additional financial considerations are critical:
Tiered pricing in assisted living: Most assisted living communities use tiered or a la carte pricing. The base rent covers a limited set of services; as care needs increase, monthly costs rise. Families often underestimate future costs by assuming the entry-level price will remain stable.
Duration of need: Only about 20% of seniors who need long-term care will need it for more than five years (LongTermCare.gov). This affects the cost-benefit calculation: a higher-cost option may be financially viable if the expected duration is short.
Detailed Comparison: Home Care vs. Assisted Living vs. Memory Care
The following table provides a side-by-side comparison across the dimensions that matter most for decision-making.
Side-by-side comparison of home care, assisted living, and memory care across key decision dimensions.
Dimension
Home Care
Assisted Living
Memory Care
Services
Personal care, homemaker services, medication reminders; no 24/7 nursing
Personal care, meals, social activities, medication management; limited nursing
All assisted living services + dementia-specific programming, behavioral management, 24/7 supervision
Staffing
Home health aides visit on schedule; family fills gaps
Staff available 24/7 but not one-on-one; typical ratio 1:8 to 1:15
Specialized dementia-trained staff; lower resident-to-staff ratios (often 1:5 to 1:8)
Safety features
Limited to what family installs (grab bars, locks, monitoring cameras)
Basic security (locked doors, call buttons); not designed for wandering
Secure exits, enclosed outdoor spaces, continuous monitoring, wander management systems
Social opportunities
Limited to family visits and community outings; risk of isolation
Structured activities, communal dining, group outings; built-in social environment
Therapeutic activities designed for cognitive impairment; smaller group settings
Medicare coverage
Limited to short-term skilled home health (Medicare-certified agency); does not cover custodial care
Does not cover room and board or ADL assistance
Does not cover room and board or custodial care
Medicaid coverage
Varies by state; some states offer home- and community-based waivers
Varies by state; some states cover assisted living through waivers
Varies by state; some states cover memory care through waivers
When Home Care Works Best (and When It Doesn't)
Home care is the right choice when the senior has mild to moderate ADL needs, stable cognition, and a family caregiver who can provide oversight during the hours the aide is not present. It allows the person to remain in a familiar environment, which can be especially important for someone with early-stage dementia who still finds comfort and orientation in their own home.
Ideal candidates for home care typically:
Need help with 1–3 ADLs (bathing, dressing, meal preparation)
Have stable or slowly progressing cognition (no wandering, no significant behavioral changes)
Have a family caregiver who lives nearby and can provide 10–20 hours of weekly oversight
Have a budget that can sustain 20–40 hours of professional care per week
Home care becomes unsustainable when:
24/7 care is needed: Around-the-clock home care requires multiple aides and costs $200,000+ per year — far more than any facility-based option.
Social isolation is a concern: Seniors who live alone with only scheduled aide visits may experience loneliness and depression. Assisted living and memory care provide built-in social engagement.
Caregiver burnout is setting in: If the family caregiver is experiencing headaches, poor sleep, anxiety, or resentment — common signs of burnout — the current arrangement may not be sustainable.
When Assisted Living Is the Right Fit (and When to Look Higher)
Assisted living is designed for seniors who need moderate daily support but do not require the intensive supervision of a memory care unit or the medical care of a skilled nursing facility. It offers a middle ground: apartment-style living with access to meals, housekeeping, social activities, and personal care assistance.
Assisted living is a good fit when the senior:
Needs help with 2–4 ADLs (bathing, dressing, medication management, meals)
Has mild cognitive decline but no significant wandering or behavioral issues
Prefers a social environment with structured activities and communal dining
Has a monthly budget of $5,000–$7,000 and can absorb future cost increases
However, assisted living has important limitations that families should understand before committing:
Tiered pricing surprises: As the resident's care needs increase — for example, from medication reminders to full assistance with bathing — monthly costs can rise by $500–$1,500 or more. A Place for Mom notes that many communities use tiered or a la carte pricing, and families often underestimate these future increases.
Limited dementia support: Most assisted living communities are not equipped to handle advanced dementia behaviors. If the resident begins wandering, sundowning, or becoming agitated, the community may require a move to memory care — often with little notice.
Staff-to-resident ratios: Typical ratios in assisted living range from 1:8 to 1:15, which means residents may wait for assistance during peak times. This is acceptable for someone who can wait, but dangerous for someone who needs immediate help with toileting or transfer.
When Memory Care Is the Only Safe Option
Memory care is not simply assisted living with a different label. It is a distinct care environment designed specifically for people with Alzheimer's disease and other dementias. The 15–25% premium over assisted living is justified by three structural differences: specialized staff training, enhanced security, and better staff-to-resident ratios.
Memory care is the right choice when the senior:
Has moderate to advanced dementia with significant cognitive decline
Exhibits wandering behavior or attempts to leave the home unsupervised
Shows behavioral changes such as agitation, aggression, or sundowning
Needs 24/7 supervision for safety — cannot be left alone even for short periods
Has experienced frequent falls or unexplained injuries at home
What the memory care premium actually pays for:
Specialized staff training: Staff receive training in dementia communication techniques, behavioral de-escalation, and non-pharmacological interventions for symptoms like sundowning and agitation.
Enhanced security: Memory care units feature secure exits, enclosed outdoor spaces (wandering gardens), and continuous monitoring systems. Some use wearable trackers or door alarms to prevent elopement.
Better staff-to-resident ratios: Memory care units typically maintain ratios of 1:5 to 1:8, compared to 1:8 to 1:15 in assisted living. This allows staff to respond more quickly to behavioral episodes and provide more individualized attention.
Structured environment: Memory care uses visual cues, consistent routines, and smaller group settings to reduce confusion and agitation. The physical layout is designed to be navigable for people with cognitive impairment.
Decision Flowchart: Matching Care Type to Your Loved One's Needs
The following decision framework synthesizes the four dimensions into a practical sequence of questions. Work through each question in order to arrive at the recommended care type.
Decision flowchart: match care type to your loved one's needs using the four-dimension assessment.
Step 1: Assess ADL Dependence
If your loved one needs help with 1–3 ADLs and can manage the rest independently → proceed to Step 2.
If your loved one needs help with 4+ ADLs or requires 24/7 assistance → skip to Step 4 (memory care or skilled nursing may be needed).
Step 2: Evaluate Cognitive Status
If cognition is stable or mildly impaired (no wandering, no significant behavioral changes) → proceed to Step 3.
If there is moderate to advanced dementia with wandering, sundowning, agitation, or safety awareness deficits → memory care is likely the safest option.
Step 3: Consider Caregiver Availability
If a family caregiver lives nearby, is available for 10–20 hours of weekly oversight, and is not experiencing burnout → home care is a viable option.
If the caregiver is long-distance, works full-time, or is also elderly → assisted living is likely a better fit.
Step 4: Evaluate Financial Resources
If the monthly budget is under $5,000 and home care is feasible → home care with limited hours may work.
If the monthly budget is $5,000–$7,000 and the senior is a good candidate for a social environment → assisted living.
If the monthly budget is $7,000+ and the senior needs specialized dementia care → memory care.
If financial resources are limited, explore Medicaid waivers, VA benefits, and other assistance programs before ruling out any option.


Comments
Join the discussion with an anonymous comment.