How to Navigate the Senior Health Care System: A Step-by-Step Guide to Finding the Right Entry Point
This guide helps overwhelmed adult children identify the right entry point into the fragmented senior health care system. It maps five key entry points—AAA/ADRC, hospital discharge planner, SHIP, geriatric care manager, and PACE—to specific trigger situations, providing a decision flowchart and calling scripts to help families access services faster.
By Editorial Team
new caregiver
care coordination
first steps
long-distance caregiving
adult children
📄
A printable version of this guide is available. Use your browser's print function (Ctrl+P / ⌘P) to save or print.
You Are Not Alone: The Senior Care Maze
If you have recently realized that a parent needs help — after a fall, a confusing hospital discharge, or a slow decline you can no longer ignore — you have likely already discovered that the senior health care system does not come with a front door. A 2022 report from Nexus Insights described long-term care navigation for families as "a maze of dead ends, wrong way streets, and twists and turns." That language resonates because it matches the experience: you call one number, get transferred to a voicemail box, call another, are told you do not qualify, and eventually give up or start over.
This guide exists to replace that experience with a clear process. The core insight is simple: the system has multiple entry points, and the right one depends entirely on your specific trigger situation. Call the wrong entry point and you waste weeks. Call the right one and you can move from confusion to a scheduled needs assessment in a matter of days.
Step 0: Identify Your Trigger Event
Before you call anyone, pause and name the specific event that prompted your search. The trigger determines which entry point is most likely to help you. Different triggers lead to different doors.
A recent hospitalization or emergency room visit. The hospital discharge planner is your primary entry point — and you should start talking to them at admission, not at discharge.
A gradual decline in function at home (trouble bathing, cooking, managing medications). Your best first call is your local Area Agency on Aging (AAA) or Aging and Disability Resource Center (ADRC) for a comprehensive needs assessment.
Confusion about Medicare coverage, bills, or plan options. The State Health Insurance Assistance Program (SHIP) offers free, in-depth counseling — and most beneficiaries do not know it exists.
A complex situation involving multiple chronic conditions, long-distance oversight, or family disagreement. A geriatric care manager (GCM) can assess the full picture and create a coordinated plan, though you will pay out of pocket.
A parent who needs nursing-home-level care but wants to stay at home. The Program of All-Inclusive Care for the Elderly (PACE) provides comprehensive medical and long-term care in a community setting for those who qualify.
The Five Core Entry Points: Which One Fits Your Situation?
Each entry point serves a different purpose, serves a different population, and has a different cost structure. The table below maps all five to the situations where they work best.
Five core entry points into the senior health care system, mapped to trigger situations, cost, and access method.
Entry Point
Best Trigger
Cost
What It Does
How to Access
AAA / ADRC
General decline at home; need for meals, transportation, in-home support
Free; no income limit
Comprehensive needs assessment; connects to home-delivered meals, caregiver support, transportation, adult day services
Call Eldercare Locator: 1-800-677-1116
Hospital Discharge Planner
Recent hospitalization or ER visit
Free (hospital-provided)
Coordinates post-discharge care; arranges home health, skilled nursing, or rehab; provides caregiver training under the CARE Act
Request at admission — do not wait until discharge day
SHIP
Medicare billing confusion; plan selection; coverage questions
Free
One-on-one counseling on Medicare, Part D, Medigap, Medicare Advantage; average session is 33 minutes
Find local SHIP at shiphelp.org or call 1-877-839-2675
Geriatric Care Manager (GCM)
Complex needs; long-distance caregiving; family conflict; multiple providers
$50–$200/hour, out-of-pocket
Full assessment; care plan creation; provider coordination; ongoing monitoring
Search Aging Life Care Association directory
PACE
Nursing-home-level need but wants to stay in community; age 55+
$4,000–$5,000/month if not on Medicare/Medicaid; Medicaid enrollees pay little or nothing
All-inclusive medical and long-term care: primary care, therapies, prescriptions, transportation, day center
Find local program at npaonline.org
Let us walk through each one in more detail so you can match your situation to the right door.
1. Area Agency on Aging (AAA) / Aging and Disability Resource Center (ADRC)
AAAs are the closest thing the system has to a general-purpose front door. They serve anyone aged 60 and older regardless of income — a common misconception is that they are only for low-income individuals, but that is not correct. According to USAging, nearly 63% of AAAs now perform ADRC functions, meaning they serve as a single point of entry into the long-term services and supports (LTSS) system. ADRCs are sometimes called "No Wrong Door" systems, designed so that no matter which agency you call first, you end up at the right place.
Call the Eldercare Locator at 1-800-677-1116 to find your local AAA. When you call, ask for a comprehensive needs assessment. This is the foundation for everything that follows.
2. Hospital Discharge Planner
If your trigger is a hospitalization, the discharge planner (often a social worker or nurse) is your most powerful ally — but only if you engage them early. The Family Caregiver Alliance emphasizes that effective discharge planning can decrease readmission rates, and the CARE Act (now law in most states) requires hospitals to record the name of the family caregiver, inform them of the discharge plan, and provide training for any medical tasks the caregiver will need to perform at home.
3. State Health Insurance Assistance Program (SHIP)
SHIPs provide free, local, in-depth counseling on Medicare, Part D, Medigap, and Medicare Advantage. A September 2025 KFF report found that SHIPs counseled approximately 4.3 million beneficiaries in 2022, with an average session length of 33 minutes — more than three times the 9.5 minutes available through 1-800-MEDICARE. Despite this, only about 1 in 5 Medicare beneficiaries know about or use SHIP services.
If your parent is confused about their coverage, facing a large bill, or trying to choose between Medicare Advantage and Medigap, SHIP is the right entry point. Federal funding for SHIP was $70 million in 2025, up from $60 million in 2015 — roughly $1 per beneficiary per year.
4. Geriatric Care Manager (GCM)
Geriatric care managers — also called aging life care managers — are usually licensed nurses or social workers who specialize in assessing older adults and coordinating care. The National Institute on Aging notes that they charge by the hour and that neither Medicare nor Medicaid pays for their services. AARP reports that hourly rates typically range from $50 to $200, and most private insurance, including Medigap and Medicare Advantage, does not cover it.
Despite the out-of-pocket cost, a GCM can save families money in the long run by aligning services to actual needs rather than trial-and-error spending. They are especially valuable for long-distance caregivers who cannot be on-site to assess the situation themselves.
5. Program of All-Inclusive Care for the Elderly (PACE)
PACE is a lesser-known but powerful option for older adults who need nursing-home-level care but want to remain in the community. According to NCOA, there are 194 PACE programs in the United States serving 87,750 participants. Eligibility requires being at least 55 years old, living near a PACE program, and being eligible for nursing home care per the state Medicaid agency. Participants receive comprehensive care including primary care, therapies, prescription drugs, hospital care, dental, and transportation — all coordinated through a single PACE center.
For those not enrolled in Medicare or Medicaid, the average cost is $4,000 to $5,000 per month. Medicare recipients pay monthly premiums for the long-term care portion, while Medicaid enrollees typically pay a small monthly fee or nothing.
How to Get a Comprehensive Needs Assessment
Regardless of which entry point you choose, the goal of your first contact should be to obtain a comprehensive needs assessment. This is a structured evaluation of your parent's physical, cognitive, social, and environmental situation. It is the foundation for every subsequent decision — what services are needed, who should provide them, and how to pay for them.
A thorough assessment typically covers:
Activities of daily living (ADLs): bathing, dressing, toileting, transferring, eating
Instrumental activities of daily living (IADLs): medication management, meal preparation, housekeeping, transportation, finances
Home safety evaluation: fall hazards, bathroom accessibility, lighting, entry/exit safety
Social support inventory: who lives nearby, who visits, who can help
Financial and insurance review: income, assets, Medicare/Medicaid eligibility
AAAs and ADRCs conduct these assessments at no cost. Geriatric care managers conduct more detailed assessments as part of their private-pay service. PACE programs conduct assessments to determine eligibility and develop a care plan. Once you have the assessment results, you can match specific services to your parent's actual needs.
Common System Navigation Pitfalls (And How to Avoid Them)
Even with the right entry point, families make predictable mistakes that slow everything down. Here are the most common ones and how to avoid them.
Being bounced between agencies. The "No Wrong Door" system is designed to prevent this, but it is not fully implemented everywhere. If an agency tells you to call a different number, ask them to transfer you or to provide a direct contact name. Do not hang up and start over.
Missing Medicare enrollment windows. The Part B late enrollment penalty is 10% for each 12-month period you could have had coverage but did not — and it is permanent. If your parent is approaching age 65 or has recently lost employer coverage, contact SHIP immediately to understand deadlines.
Not knowing about ADRCs. Many families call their local AAA and get help, but do not realize that ADRCs exist as a single point of entry that also serves younger adults with disabilities. If your parent is under 60 or has a disability, ask specifically for the ADRC.
Assuming AAAs are only for low-income individuals. AAAs serve anyone aged 60 and older regardless of income. Services like information and referral, caregiver support, and health promotion are available to all. Means-tested programs (like Medicaid-funded home care) are a subset of what AAAs offer, not the whole picture.
Not asking for CARE Act rights during hospitalization. The CARE Act requires hospitals to record your name as the family caregiver, inform you of discharge plans, and provide training for medical tasks. Most families do not know to request this. Ask the discharge planner: "Can you document me as the family caregiver and provide training before discharge?"
Not knowing about the QIO appeal process. If you believe your parent is being discharged too early, you have the right to request a review by the Quality Improvement Organization before leaving the hospital. The hospital cannot discharge until the appeal is completed.
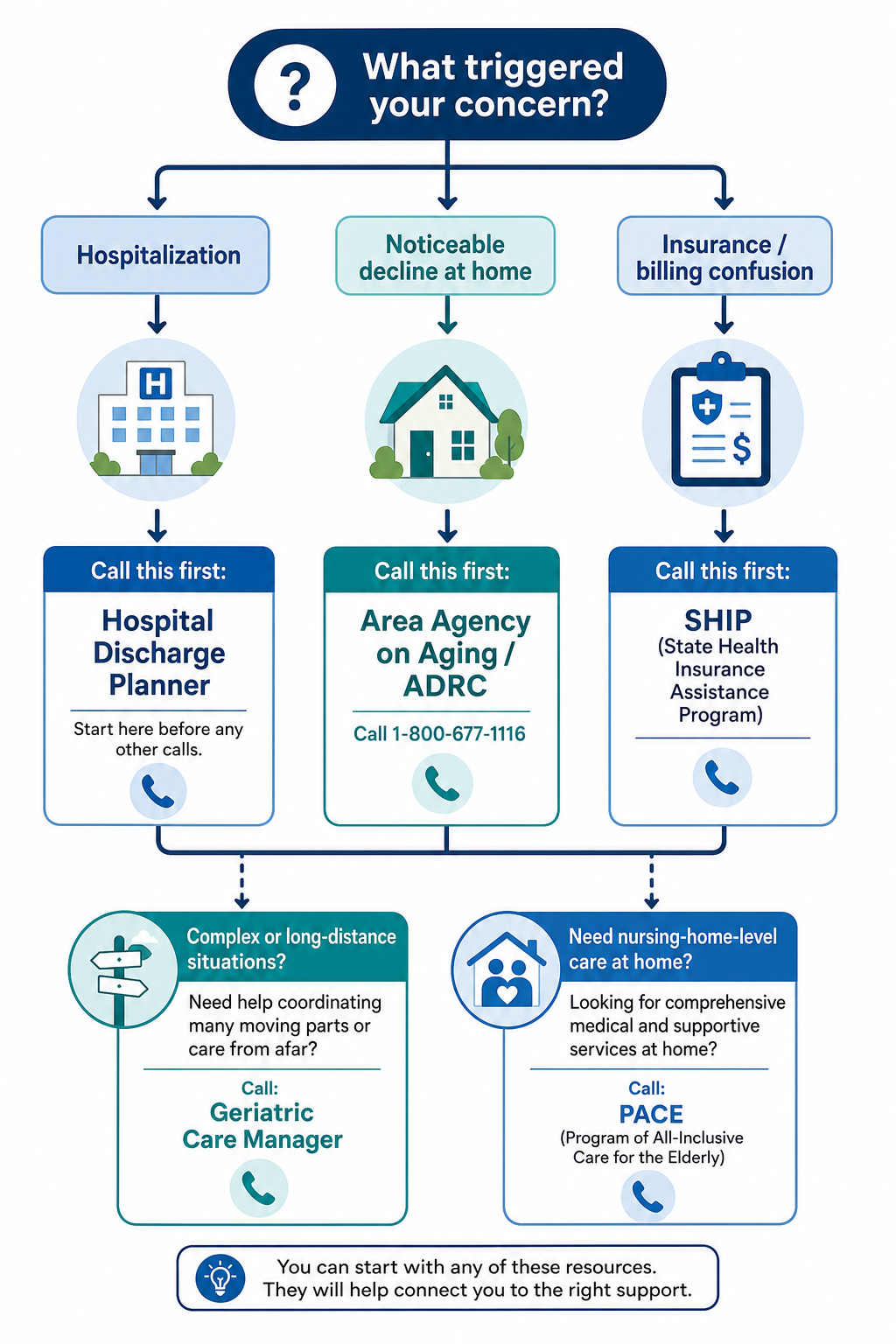
Decision Flowchart: Which Entry Point Should You Call First?
Use this flowchart to identify your first call based on your trigger event.
The flowchart above distills the decision process into three primary paths:
If the trigger is a hospitalization or ER visit, start with the hospital discharge planner. Ask for a needs assessment and caregiver training before discharge. Follow up with your local AAA for community-based support after discharge.
If the trigger is a noticeable decline at home (trouble with meals, bathing, mobility, or memory), call the Eldercare Locator at 1-800-677-1116 to find your local AAA or ADRC. Request a comprehensive needs assessment.
If the trigger is insurance confusion, billing problems, or plan selection, contact SHIP. Find your local program at shiphelp.org.
For complex situations — multiple chronic conditions, long-distance caregiving, family disagreement, or a parent who needs nursing-home-level care but wants to stay home — consider adding a geriatric care manager or exploring PACE as a secondary step after the initial assessment.
Step-by-Step Pathway: From First Concern to First Service Engagement
Here is a realistic timeline from the moment you recognize a need to the point of first service engagement. The timeline assumes you are calling the correct entry point for your situation.
Realistic timeline from first concern to first service engagement, assuming correct entry point selection.
Stage
Action
Typical Timeline
Day 1
Identify trigger event. Call Eldercare Locator (1-800-677-1116) or contact hospital discharge planner if hospitalized.
Same day
Day 1–3
Speak with AAA/ADRC intake worker. Describe the situation. Schedule a comprehensive needs assessment.
1–3 days
Day 3–14
Complete the needs assessment (in-person or by phone). Receive a list of recommended services and provider contacts.
1–2 weeks
Day 14–21
Contact recommended providers. Schedule in-home care, meals, transportation, or other services. If using a GCM, they will handle this coordination.
1–2 weeks
Day 21–30
First services begin. Reassess after 30 days to determine if the level of support is adequate or needs adjustment.
Ongoing
If you are using a geriatric care manager, the timeline may compress because the GCM handles assessment and provider coordination simultaneously. If you are entering through PACE, the timeline may extend slightly due to eligibility verification and enrollment processes.
Key Resources and Calling Scripts
Use the following phone numbers, websites, and scripts to make your first calls with confidence. Services vary by state and county, so always confirm local availability.
Key national resources for navigating the senior health care system.
Resource
Contact
Best For
Eldercare Locator
1-800-677-1116 (Mon–Fri, 9am–8pm ET)
Finding your local AAA or ADRC
SHIP Locator
shiphelp.org or 1-877-839-2675
Finding local Medicare counseling
PACE Locator
npaonline.org
Finding a PACE program near you
Meals on Wheels America
1-888-998-6325
Home-delivered meals
Aging Life Care Association
aginglifecare.org
Finding a geriatric care manager
Calling Script: Contacting Your Local AAA or ADRC
"Hello, I am calling because my [mother/father/spouse] is [briefly describe the situation — e.g., having trouble with bathing and cooking, recently fell, seems confused]. I was told you can do a comprehensive needs assessment to help us figure out what services might help. Can you help me schedule an assessment?"
Calling Script: Requesting a Hospital Discharge Planner
"My [mother/father/spouse] was admitted today. I am the family caregiver. I would like to speak with the discharge planner or social worker to start planning for discharge. Can you connect me? Also, I would like to be recorded as the family caregiver under the CARE Act so I can receive training before discharge."
Calling Script: Contacting SHIP
"I am helping my [mother/father/spouse] with Medicare and I am confused about [bills/plan options/coverage for a specific service]. I understand SHIP offers free counseling. Can I schedule a one-on-one appointment to review our situation?"
You now have a clear process: identify your trigger, choose the right entry point, request a comprehensive assessment, and follow the timeline to first service engagement. The system is fragmented, but it is navigable — especially when you know which door to walk through first.

Comments
Join the discussion with an anonymous comment.