Senior Care Options: A Complete Decision Framework Based on ADL and IADL Needs
By Editorial Team
ADLs
IADLs
assisted living
memory care
home care
Why Most Families Compare Apples to Oranges When Choosing Senior Care
When a parent falls, receives a dementia diagnosis, or experiences a sudden functional decline, the instinct is to act fast. Families typically open a browser, search for local facilities, and begin comparing monthly rates, amenities, and star ratings. This approach is backward — and it is the single most common mistake caregivers make.
The problem is not a lack of options. It is that families compare options across different care levels before determining which level their loved one actually needs. Comparing a high-end assisted living community to a basic home care agency is like comparing a sedan to a moving truck — both get you from point A to point B, but they serve fundamentally different purposes. The result is wasted time, emotional distress, and often thousands of dollars spent on the wrong type of care.
This guide provides a unified framework that prevents that mistake. Instead of starting with facility names or prices, you will start with a functional assessment of your loved one's abilities. By matching specific deficits in Activities of Daily Living (ADLs) and Instrumental Activities of Daily Living (IADLs) to the correct care tier, you can lock in the right level of support before you ever compare a single monthly bill.
The stakes are high. According to CareScout's 2025 Cost of Care Survey, 7 out of 10 people will require long-term care in their lifetime, and every day until 2030, 10,000 Baby Boomers turn 65. Making the right decision early — before a crisis forces a rushed choice — preserves both financial resources and the senior's autonomy.
ADLs and IADLs: The Foundation of Any Care Decision
Before you can match a senior to the right care level, you need a clear picture of what they can and cannot do independently. That is where ADLs and IADLs come in. These two frameworks are the standard tools used by healthcare professionals, social workers, and insurance assessors to determine functional need.
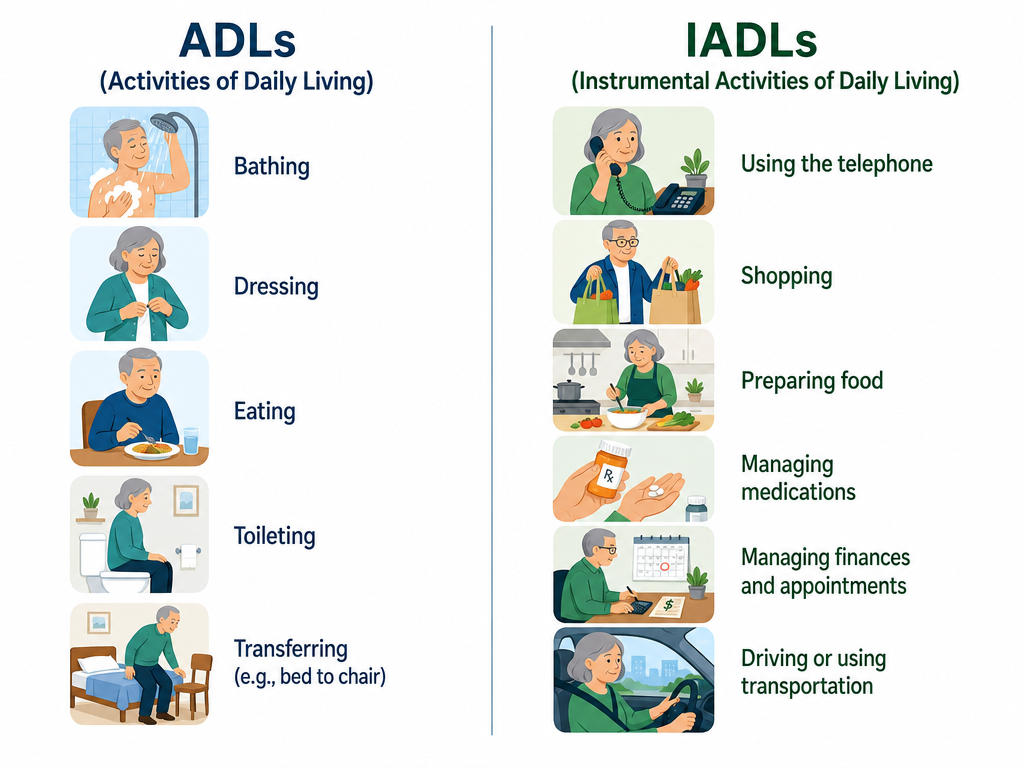
Activities of Daily Living (ADLs)
ADLs are the basic self-care tasks that people perform every day. The six core ADLs are:
Bathing — washing the body independently
Dressing — selecting and putting on clothing
Eating — feeding oneself (not including meal preparation)
Toileting — using the bathroom and managing hygiene
Transferring — moving between bed, chair, and standing position
Continence — controlling bladder and bowel functions
A senior who needs help with one or two ADLs may still be able to live at home with modest support. A senior who needs help with three or more ADLs typically requires a higher level of daily assistance.
Instrumental Activities of Daily Living (IADLs)
IADLs are more complex tasks that support independent living in the community. The seven core IADLs are:
Using the telephone or other communication devices
Shopping for groceries and essentials
Preparing meals
Managing medications (dosages, timing, refills)
Managing finances (bills, banking, budgeting)
Arranging transportation
Performing housework and home maintenance
IADL deficits often appear before ADL deficits. A senior who can no longer manage medications or pay bills may still be able to bathe and dress independently. That is why assessing both sets of functions is essential — IADL deficits alone may point toward in-home support services, while ADL deficits signal the need for hands-on personal care.
ADLs and IADLs: the two assessment frameworks that determine the correct care level.
The Full Care Spectrum: A Tiered Map from In-Home Care to Skilled Nursing
Senior care is not a binary choice between "stay at home" and "move to a facility." It is a spectrum with six distinct tiers, each designed for a specific range of functional needs. Understanding where each tier sits on this spectrum is the first step toward matching your loved one to the right level of support.
The full senior care spectrum, from lowest support (in-home care) to highest support (skilled nursing).
1. In-Home Care (Non-Medical)
Non-medical home care provides a caregiver who assists with ADLs and IADLs in the senior's own home. Services include bathing, dressing, meal preparation, light housekeeping, medication reminders, and companionship. This tier is best for seniors who are safe at home but need help with specific tasks for a set number of hours per week. It does not include skilled nursing or medical care.
2. Adult Day Services
Adult day centers provide structured social activities, meals, and supervision during daytime hours. Some offer basic health monitoring and medication management. This option works well for seniors who live with a family caregiver during evenings and weekends but need supervision and engagement during the workday. It also provides respite for working caregivers.
3. Independent Living
Independent living communities (also called retirement communities or 55+ housing) offer apartment or cottage living with shared amenities, dining options, and social activities. They do not provide personal care or medical services. This tier is appropriate for seniors who are fully independent in ADLs and IADLs but want to downsize, reduce home maintenance responsibilities, and live among peers.
4. Assisted Living
Assisted living facilities provide apartment-style living with 24-hour staff, meals, housekeeping, transportation, and assistance with ADLs. Residents typically need help with two or more ADLs but do not require round-the-clock skilled nursing. Assisted living bridges the gap between independent living and nursing home care. It is the most common residential option for seniors who can no longer live safely at home but do not need a hospital-level environment.
5. Memory Care
Memory care is a specialized subset of assisted living designed for individuals with Alzheimer's disease or other dementias. These units feature secure environments (locked doors, enclosed gardens), specially trained staff, structured programming, and lower resident-to-staff ratios. Memory care costs 20–30% more than standard assisted living due to these additional safety and staffing requirements. According to the Alzheimer's Association, 6 out of 10 people with dementia will wander, making secure environments a safety necessity rather than a luxury.
Skilled nursing facilities provide 24/7 medical care under the supervision of licensed nurses and physicians. Residents typically have complex medical needs, require rehabilitation after a hospital stay, or need assistance with all or most ADLs. This is the highest level of care outside of a hospital. Nursing homes are licensed by the state and regulated by the federal government.
How ADL and IADL Deficits Map to the Right Care Level
Once you have assessed your loved one's ADL and IADL deficits, the next step is mapping those deficits to the appropriate care tier. The table below provides a general decision rule. Individual needs vary, and a professional assessment from a geriatric care manager or social worker is always recommended before making a final decision.
Mapping ADL and IADL deficits to the appropriate care level.
Functional Profile
Recommended Care Level
Rationale
0 ADL deficits, 0–2 IADL deficits
Independent Living
Senior can manage daily self-care and most complex tasks; needs minimal support
0–1 ADL deficits, 2–4 IADL deficits
In-Home Care or Adult Day Services
Needs help with complex tasks and occasional personal care; can remain at home with scheduled support
2–3 ADL deficits, 3+ IADL deficits
Assisted Living
Requires daily hands-on assistance with personal care and supervision of complex tasks
2–4 ADL deficits, dementia diagnosis
Memory Care
Needs personal care assistance plus secure environment and dementia-trained staff
4+ ADL deficits, complex medical needs
Skilled Nursing Facility
Requires 24/7 nursing care and assistance with nearly all daily activities
The 40-Hour Break-Even Threshold: Home Care vs. Assisted Living
One of the most common decision points families face is choosing between in-home care and assisted living. The conventional wisdom is that home care is cheaper, but that is only true up to a point. Based on CareScout's 2025 Cost of Care Survey data, the break-even threshold is approximately 40 hours of care per week.
At the national median rate of $35 per hour for non-medical home care, 40 hours per week costs roughly $6,062 per month. The national median for assisted living is $6,200 per month — nearly identical. Below 40 hours per week, home care is less expensive. Above 40 hours, assisted living's all-inclusive flat rate becomes more cost-effective. At 24/7 care (168 hours per week), hourly home care would cost approximately $5,544 per week, while assisted living remains at roughly $1,475 per week.
The following cost table uses data from CareScout's 2025 Cost of Care Survey (fielded July–November 2025), which provides the most current national median figures available. Memory care costs are cited from two sources to reflect the range in published data.
2026 national median costs for each senior care level. Memory care figures differ between sources due to different survey periods and methodologies.
Once you have identified the correct care level, you can begin comparing specific providers or facilities using consistent criteria. This is the "compare within the same level" rule, and it prevents the apples-to-oranges mistake that derails so many care decisions.
When comparing options within the same care tier, evaluate each option using the same set of criteria:
Staff-to-resident ratios and staff turnover rates
Scope of included services vs. à la carte add-ons
Location and proximity to family members
Quality ratings from Medicare Care Compare or state survey agencies
Availability of specialized care (e.g., dementia programming, rehabilitation therapy)
Contract terms, entrance fees, and refund policies
For example, if your loved one needs assisted living, compare two assisted living facilities against each other — not an assisted living facility against a home care agency. The latter comparison will always be misleading because the two options serve different functional needs and have fundamentally different cost structures.
The flowchart below summarizes the decision process outlined in this guide. Start by counting your loved one's ADL and IADL deficits, then follow the branching questions to identify the recommended care level.
Decision flowchart for matching ADL/IADL deficits to the correct senior care level.
This flowchart is a starting point, not a substitute for a professional assessment. A geriatric care manager, social worker, or primary care physician can provide a formal evaluation that accounts for medical complexity, cognitive status, and caregiver capacity — factors that a simple deficit count cannot capture.
Payment Sources: What Covers What
Understanding how to pay for care is often the most stressful part of the decision process. The table below summarizes the major payment sources and what they cover. Note that coverage rules vary by state and plan, and the information below reflects national general guidelines as of 2026.
Major payment sources for senior care and their coverage limitations.
Payment Source
What It Covers
Key Limitations
Medicare (Part A)
Skilled nursing facility care after a 3+ night hospital stay: days 1–20 fully covered, days 21–100 with daily copay (~$200–$217/day in 2026)
Does not cover custodial care (assistance with ADLs), long-term residential care, or room and board in assisted living or memory care
Medicaid
Primary payer for long-term care in nursing homes after asset spend-down; some states offer home- and community-based waivers for in-home care and assisted living
Eligibility requires meeting income and asset limits; coverage and waiver programs vary significantly by state
VA Aid & Attendance
Monthly pension supplement for veterans and surviving spouses who need assistance with ADLs
Single veteran up to $2,424/month; married veteran up to $2,874/month; surviving spouse up to $1,558/month (American Council on Aging, 2025)
Long-Term Care Insurance
Covers a daily or monthly benefit for in-home care, assisted living, memory care, or nursing home care, depending on the policy
Must be purchased before care is needed; policies vary widely in benefit amounts, elimination periods, and covered services
Out-of-Pocket / Private Pay
Covers any care level not paid by insurance or government programs
Most families pay out of pocket for assisted living and memory care, as Medicare does not cover these settings



Comments
Join the discussion with an anonymous comment.