Navigating Senior Health Care: How to Coordinate Your Parent’s Care Without Burning Out
Healthcare coordination — not hands-on care — is the primary hidden driver of caregiver burnout. A structured navigation protocol can reduce this burden, improve communication with providers, and help families avoid costly insurance pitfalls.
- Last Reviewed
- 2026-06-30
- caregiver burnout
- respite care
- caregiver guilt
- emotional support
- working caregiver
- driving cessation conversation
- accepting help
- role reversal
- caregiver stress
- self-care
- difficult conversations
- caregiver identity
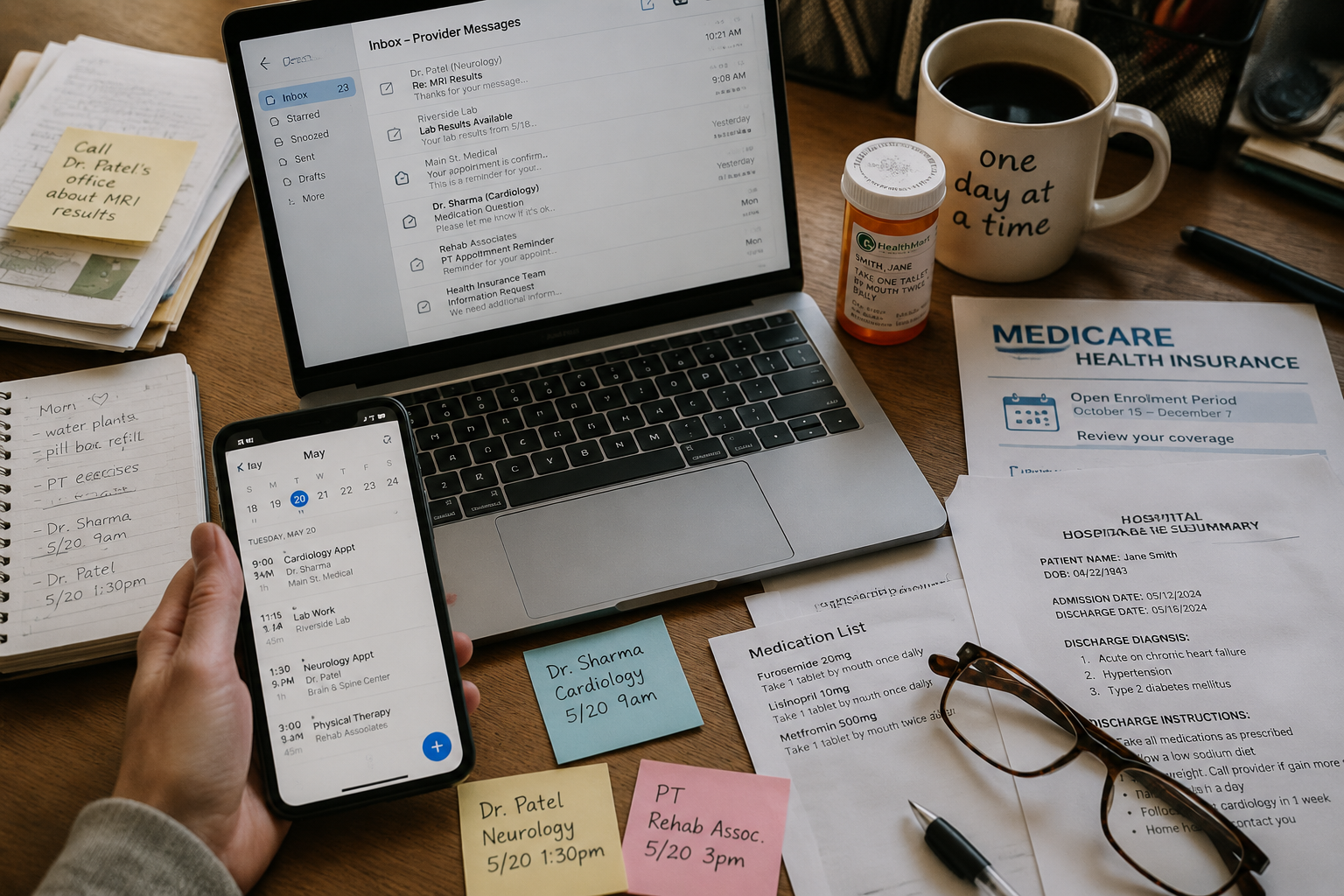
The moment senior health care starts to take over your life is often not the dramatic moment people picture. It is the Tuesday night when your parent’s cardiology portal says one thing, the hospital discharge papers say another, the pharmacy has a third version of the medication list, and your sibling texts, “Did anyone call insurance?” while you are still answering work email.

That is the part families rarely name accurately. Bathing, meals, rides, and errands are real work. But for many adult children, the job that breaks the week is coordination: remembering who changed which dose, which specialist wanted labs repeated, which facility sent a notice, which form still needs a signature, and which family member has only heard half the story.
Caregiver burnout is not just a vague feeling of being tired. Cleveland Clinic describes it as emotional, mental, and physical exhaustion that can come with withdrawal from friends and family, loss of interest in activities, irritability, changes in sleep or appetite, getting sick more often, and feeling hopeless or helpless. It also states that more than 60% of caregivers experience symptoms of burnout.[1] That number matters because coordination often looks harmless from the outside. It is “just a call,” “just one appointment,” “just checking the portal.” Stacked together, those small tasks become a second operations job.
Work makes that load harder to absorb. AARP has reported that 73% of family caregivers work full- or part-time.[2] So when a clinic leaves a voicemail at 11:18 a.m., the caregiver is not sitting beside a landline with a notebook. They may be in a meeting, driving, on a deadline, or trying not to explain to a supervisor why another lunch hour disappeared into hold music.
If you are already in crisis mode after a hospitalization or sudden diagnosis, start with a shorter emergency path: the 72-hour caregiver checklist can help you stabilize the first few days. The rest of this guide is for building the system you wish you had before the crisis.
First, make the invisible job visible
A care team is not just the people with medical degrees. The National Institute on Aging describes services for older adults living at home as a mix of medical care, personal care, transportation, meal support, household help, money management, and other practical supports.[3] That wider view is useful because most family coordination failures happen between categories, not inside one appointment.
A primary care doctor may assume the specialist explained the medication change. The specialist may assume the discharge summary reached the primary care doctor. The pharmacy may see two active prescriptions and fill the one still valid in its system. The insurer may mail a notice that no clinician has seen. The senior may answer each person politely and forget which instruction replaced the last one.
The family caregiver becomes the bridge by default. Not because anyone held a meeting and assigned the role, but because somebody has to notice when the pieces do not match. The goal is not to become a medical expert. It is to stop making one tired person’s memory the only place where the whole system exists.

Use one coordination protocol, not a pile of good intentions
The protocol can be simple. It does not need a paid app, a color-coded binder, or a Sunday night family meeting that collapses by week two. It needs five working parts that everyone agrees to use.
| Part of the protocol | What it prevents |
|---|---|
| Shared care map | One person being the only one who knows every doctor, service, and family role |
| Medication and diagnosis record | Duplicate prescriptions, outdated lists, and confused appointment answers |
| Appointment-and-question workflow | Wasted visits, forgotten concerns, and unclear next steps |
| Insurance and discharge file | Missed deadlines, unsafe transitions, and lost documentation |
| Escalation point | Waiting too long to ask for outside help |
Build a shared care map
Start with a one-page map. Put your parent’s name, date of birth, emergency contacts, primary care clinician, specialists, pharmacy, preferred hospital, home health agency if there is one, and insurance plan information in one place. Add family roles beside names, not vague promises. One person handles appointments. One handles medication list updates. One handles insurance calls. One handles transportation, if available.
This map should live somewhere shared: a secure family document, a printed folder in your parent’s home, or both. The exact format matters less than the rule that no major contact or responsibility lives only in a text thread. If you are also managing aides, meal delivery, transportation, or home services, the narrower in-home services coordination guide can sit beside this health care map.
Keep one medication and diagnosis record
The medication list is where many families discover whether their coordination system is real. It should include medication name, dose, schedule, reason for taking it, prescribing clinician, start date if known, recent stop date if relevant, allergies, over-the-counter drugs, supplements, and the pharmacy used. Bring it to every appointment and ask directly: “Is this still the list you want us following?”
The diagnosis record can be short. List the active conditions that affect care decisions, such as heart disease, diabetes, dementia, kidney disease, stroke history, serious falls, or major surgeries. If medical language starts turning into a fog bank, use a reference such as the medical glossary for seniors instead of pretending everyone understands the same terms.
After any hospital stay, emergency visit, medication change, or specialist appointment, update the record before the paperwork disappears into a tote bag. This is not clerical neatness. It is how the next clinician, pharmacist, home health nurse, or family member avoids working from stale information.
Run appointments with a question workflow
Before the visit, collect questions in one place. Separate them into three groups: symptoms or changes, medication questions, and decisions that need an answer. Do not bring eight people’s concerns as eight separate text screenshots. Turn them into a short list the clinician can actually address.
- What changed since the last visit?
- Which medications changed, stopped, or stayed the same?
- What should we watch for before the next visit?
- Who do we call for urgent concerns, and who handles routine questions?
- What is the next concrete step, and by when?
During the visit, write down decisions in plain language. After the visit, send the family a short update with only what changed and what happens next. If nothing changed, say that too. Silence creates extra work because people start filling gaps with guesses.
Insurance and discharge decisions need their own folder
Insurance paperwork is not separate from care. It can decide whether a rehab stay continues, whether home health starts, whether equipment arrives, and whether your parent is sent home before the family understands what “safe” is supposed to mean. Keep insurance cards, plan names, member numbers, prior authorization notices, denial letters, appeal instructions, discharge summaries, therapy notes, and names of people you spoke with in one folder.

This is especially important when your parent has Medicare Advantage. Provider Magazine reported in Summer 2026 that, according to Acentra Health findings cited in its investigation, 92% of Medicare Advantage non-coverage notices it reviewed involved beneficiaries who still required skilled nursing care, and 72% of those beneficiaries were at risk if discharged early.[4] That is a secondary report of Acentra’s findings, not an independently verified data set in this article. Still, it is a strong warning about the practical burden families can face when coverage decisions and clinical readiness do not line up cleanly.
Original Medicare and Medicare Advantage do not work the same way. A family does not need to become an insurance-law department, but someone does need to know which plan your parent has, whether a service requires prior authorization, what appeal deadlines apply, and who can explain the notice in plain language. During discharge planning, ask for the decision in writing and ask who determined that the discharge or coverage change is appropriate.
- Before discharge: ask what care your parent still needs and who is responsible for arranging it.
- Before signing papers: ask whether any service, rehab stay, home health visit, medication, or equipment is being denied, shortened, or delayed.
- If you receive a non-coverage notice: record the date and time received, the appeal deadline, and the phone number listed.
- If home is not ready: say specifically what is unsafe, such as no caregiver available overnight, stairs, missing equipment, wound care, confusion, or fall risk.
- After discharge: compare the medication list from the facility with the pre-hospital list and pharmacy records.
For lower-cost help, start with the hospital discharge planner or social worker, your local Area Agency on Aging, a State Health Insurance Assistance Program counselor, and any employer Employee Assistance Program available to you or another family member. These are not magic doors. They are often busy, and you may still need to call twice. But they are the right first calls before assuming the only answer is private-pay navigation.
Divide the communication job before it divides the family
Family conflict often shows up as personality conflict, but underneath it is usually an information design problem. One person has all the context. Another only hears bad news. A third wants updates but cannot attend appointments. Someone else gives advice without having read the discharge summary. Resentment grows because the work is not visible until it fails.
Make the communication rules boring and explicit. One family update after each major appointment. One shared place for documents. One person authorized to call each provider or insurer when possible. One backup person who can step in for a week without needing a two-hour briefing.
The backup matters. If the main caregiver gets sick, travels, has a work deadline, or simply hits a wall, the system should not collapse because every password, portal message, medication change, and appeal deadline lived in one person’s head.
Know when the family system is no longer enough
Some situations need more than a shared document and a responsible sibling. Consider outside help when your parent has repeated hospitalizations, rapid cognitive decline, unsafe discharge plans, multiple specialists who disagree, complex medication changes, long-distance family members, or insurance decisions you do not understand in time to act.
A geriatric care manager can assess needs, coordinate services, attend appointments, communicate with family, and help plan care. AARP recommends asking candidates about credentials, licensing, experience with your parent’s condition, availability in emergencies, fees, written care plans, and how they communicate with families.[5] The uncomfortable part is cost: geriatric care managers commonly charge $100 to $200 per hour out of pocket.[5] For many families, that is not a sustainable weekly solution.
Care navigators are another option. Trualta describes care navigators as professionals who help families understand care needs, find resources, coordinate services, and reduce the administrative burden of caregiving.[6] Depending on the program, a navigator may be available through a health system, insurer, employer benefit, community agency, or private service. The useful question is not what title the person uses. It is whether they can take a real task off your list.
If private help is out of reach, still escalate. Ask the hospital social worker for a safer discharge plan. Ask the Area Agency on Aging what programs exist locally. Ask a SHIP counselor to explain Medicare choices or notices. Ask your employer whether an EAP includes eldercare consultation. Ask the clinic whether a nurse, social worker, pharmacist, or care coordinator can review the medication list or care plan.
Burnout signs are coordination data, too
If you are snapping at people, sleeping badly, forgetting ordinary tasks, avoiding friends, getting sick more often, or feeling trapped, do not treat that only as a character flaw or a failure of gratitude. Cleveland Clinic includes many of these patterns among caregiver burnout symptoms.[1] In a coordination-heavy caregiving role, they may also be evidence that the system has exceeded one person’s capacity.
That does not mean a spreadsheet cures burnout. It means the first practical response is to remove work from your head and put it somewhere other people can see, share, and challenge. If the emotional and physical strain is already high, use a separate track such as the caregiver self-care barrier checklist to look at sleep, medical care, respite, boundaries, and support.
Families cannot make senior health care simple. They can, however, stop letting its fragmentation live entirely inside one caregiver’s head. A shared care map, a current medication record, a repeatable appointment workflow, a real insurance folder, and a named escalation path will not remove every hard decision. They will make the work visible enough to divide before it burns through the person holding it together.
References
- Caregiver Burnout, Cleveland Clinic, https://my.clevelandclinic.org/health/diseases/9225-caregiver-burnout
- Caregiving in the U.S. 2025, AARP and National Alliance for Caregiving, https://www.aarp.org/caregiving/data-research/all/caregiving-in-the-us-2025/
- Services for Older Adults Living at Home, National Institute on Aging, https://www.nia.nih.gov/health/caregiving/services-older-adults-living-home
- Seniors Needing Care Struggle to Navigate Medicare Advantage, Provider Magazine, Summer 2026, https://www.providermagazine.com/Issues/2026/Summer/Pages/Seniors-Needing-Care-Struggle-to-Navigate-Medicare-Advantage.aspx
- Geriatric Care Managers: A Guide for Family Caregivers, AARP, https://www.aarp.org/caregiving/basics/geriatric-care-manager/
- Care Navigators: Everything You Need to Know, Trualta, https://www.trualta.com/resources/blog/care-navigators-everything-you-need-to-know/
Continue Your Caregiving Journey
When you are ready, these resources can help with specific caregiving tasks.
- A Five-Domain Caregiver Self-Care Checklist: Where to Focus This Week
Most self-care lists give you vague advice. This five-domain checklist helps you spot the area of your life you have been neglecting and gives you one concrete action to take this week.
- Having the Hard Conversations: A Guide for Adult Children on Talking to Aging Parents About Driving, Finances, Memory, and Moving
A practical, script-based guide for adult children who need to initiate emotionally charged conversations with aging parents about driving, memory, finances, and moving. Learn a collaborative framework and specific approaches for eight common difficult topics.
- The True Cost of Elderly Care: What $34 Per Hour Doesn't Tell You About the Hidden Financial Burden on Family Caregivers
The $34–$35/hr headline cost of professional in-home care masks a much larger financial story for family caregivers. This article reveals the hidden costs — lost wages, depleted savings, and reduced retirement — that can dwarf the hourly rate, and provides a budgeting framework and resources to help adult children navigate the full financial picture.
Comments
Join the discussion with an anonymous comment.