The Adult Child Caregiver’s First 30 Days: A Staged Action Plan When a Parent Needs Help
stage guideReviewed: 2026-06-20
The Adult Child Caregiver’s First 30 Days: A Staged Action Plan When a Parent Needs Help
A week-by-week action plan for adult children (ages 40–55) who have recently realized their parent can no longer manage independently. This guide breaks the critical first month into four distinct stages — needs assessment, legal and financial triage, care team building, and self-care scaffolding — to help you move from crisis mode to a sustainable care rhythm.
By Editorial Team
new caregiver
first steps
ADLs
IADLs
care coordination
caregiver burnout
respite care
difficult conversations
Why the First 30 Days Are the Most Dangerous Moment in Caregiving
The call comes in a dozen different forms. A neighbor reports that your mother’s mail is piling up. A sibling mentions that Dad seems confused about his medications. An emergency room doctor explains that a fall has broken your father’s hip. However it arrives, the moment when an adult child realizes a parent can no longer manage independently is a rupture — a before-and-after line that splits life into two distinct eras.
What happens in the weeks immediately following that rupture determines the trajectory of the entire caregiving journey. And the evidence suggests that most families enter this period unprepared. According to a February 2026 Pew Research Center survey of 8,750 U.S. adults, 24% of those with a parent age 65 or older already identify as caregivers — a figure that rises to 31% when the parent is 75 or older. Yet nearly half (47%) of all family caregivers receive no formal support, and 88% say they need more help than they are getting, according to a 2024 SeniorLiving.org survey of 1,765 unpaid caregivers.
The four-stage framework that follows — needs assessment, legal and financial triage, care team building, and self-care scaffolding — converts the vague and terrifying first month into four concrete weekly sprints. Each stage has a distinct focus, a clear endpoint, and a specific set of actions that build on the stage before it. The goal is not to solve every problem in 30 days. The goal is to move from crisis mode to a sustainable care rhythm before the weight of unstructured caregiving has a chance to do lasting damage.
Stage 1 (Days 1–7): Conduct a Functional Needs Assessment
The single most common mistake new caregivers make is skipping assessment and jumping straight to solutions. A sibling suggests a home health aide before anyone has clarified whether the parent needs help with bathing or with bill-paying — two entirely different problems requiring entirely different responses. The evidence-based starting point, as documented in the comprehensive Annual Review of Psychology article by Schulz and Beach (2020), is a structured needs assessment using two established frameworks: Activities of Daily Living (ADLs) and Instrumental Activities of Daily Living (IADLs).
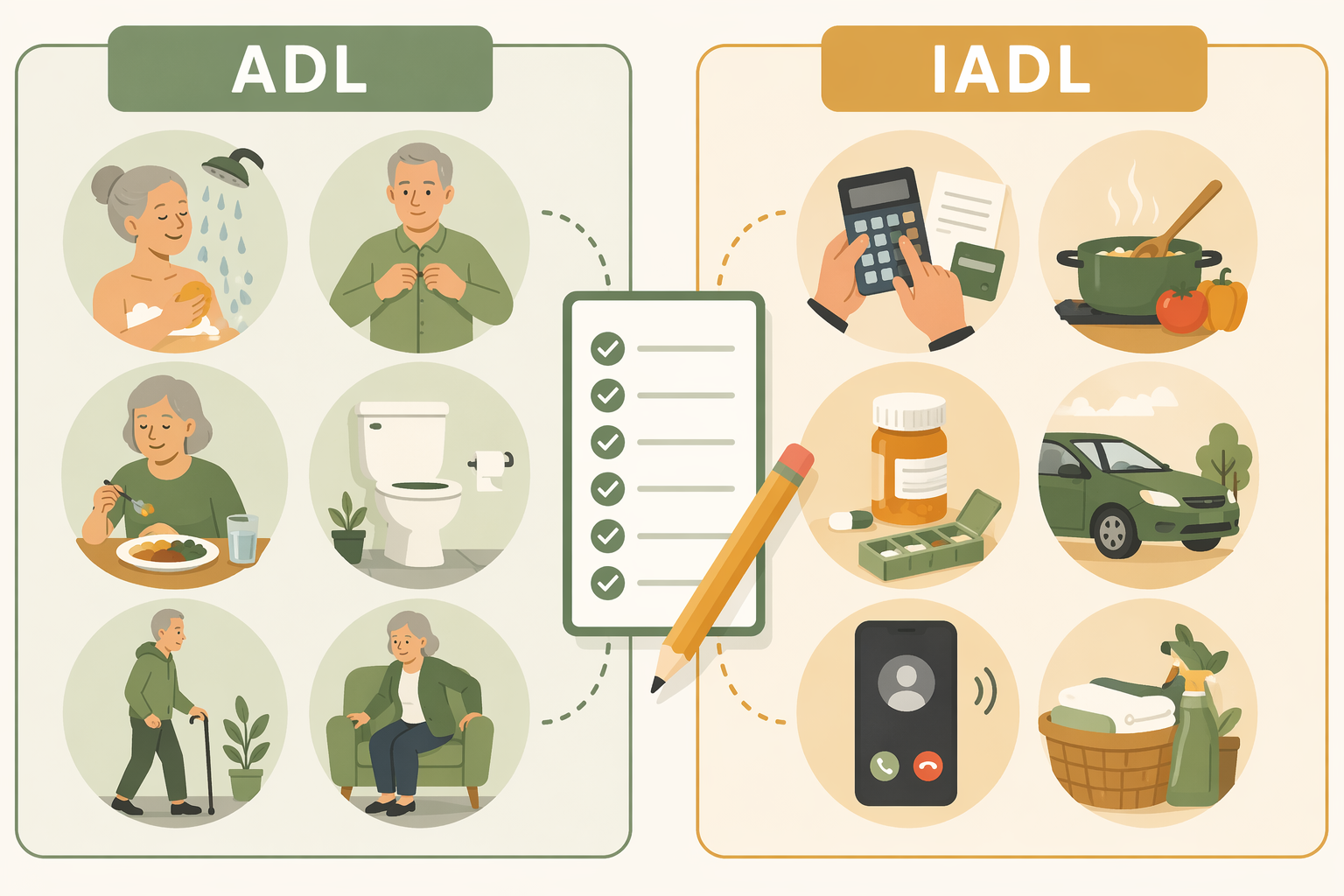
The ADL and IADL frameworks provide the evidence-based vocabulary for assessing what a parent can and cannot do independently.
ADLs are the fundamental self-care tasks that a person must be able to perform to live independently: bathing, dressing, eating, toileting, transferring (moving from bed to chair, for example), and maintaining continence. IADLs are the more complex activities that support independent living in the community: managing finances, preparing meals, managing medications, using transportation, using the telephone or other communication devices, shopping, and housekeeping.
During the first week, your task is to observe and document — not to decide. Use the following structure to organize your observations.
Key ADL and IADL domains to assess during the first week, with observable signs of difficulty.
Domain
Specific Tasks to Observe
Signs of Difficulty
Bathing
Getting in and out of the tub or shower; washing all body areas
Unwashed appearance; fear of falling in the bathroom; skipped baths
Dressing
Selecting appropriate clothing; fastening buttons and zippers
Wearing the same clothes repeatedly; mismatched or inside-out garments
Mobility
Walking across a room; getting up from a chair; climbing stairs
Using furniture for support; hesitation at stairs; recent falls
Toileting
Getting to and from the toilet; cleaning oneself
Urine odor; soiled clothing; accidents reported by the parent
Medication management
Taking the correct dose at the correct time; refilling prescriptions
Missed doses; expired medications; confusion about pill schedules
Meal preparation
Planning and cooking meals; using kitchen appliances safely
Spoiled food in the refrigerator; weight loss; reliance on microwave meals
Financial management
Paying bills on time; tracking account balances; avoiding scams
Unopened bills; late notices; unusual spending patterns
The National Institute on Aging offers downloadable caregiver worksheets that include structured ADL and IADL checklists. Print one for each domain and use it as a reference during quiet observation — not during a formal interview, which can feel threatening to a parent who is already anxious about losing independence.
As you assess, pay particular attention to home safety and fall risk. The CDC reports that falls are the leading cause of fatal and non-fatal injuries among older adults, and the majority of falls occur at home. If you observe tripping hazards (loose rugs, cluttered pathways, poor lighting) or mobility challenges (difficulty navigating stairs, unsteady gait), note them for action in later stages. Our comprehensive fall prevention guide provides room-by-room checklists that can be used in Stage 3 when the care team is in place.
By the end of Day 7, you should have a written list of which ADLs and IADLs your parent can perform independently, which require assistance, and which are no longer safe to attempt alone. This list is the foundation for every decision that follows.
Stage 2 (Days 8–14): Legal and Financial Triage
With the needs assessment complete, Week 2 shifts to the legal and financial infrastructure that must be in place before any care plan can be executed. This is the stage that most families delay — and the delay carries real consequences. Without medical power of attorney, a hospital may refuse to share information about your parent’s condition. Without financial power of attorney, you may be unable to pay bills or access funds needed for care. Without advance directives, your parent’s end-of-life preferences may go unhonored.
The task list for Week 2 is concrete and finite:
Locate and organize essential documents. This includes: medical power of attorney (also called healthcare proxy), financial power of attorney, advance directives (living will), last will and testament, all insurance policies (health, Medicare, Medigap, long-term care, life), Social Security card, and any trust documents. Keep originals in a secure location and digital copies in a shared folder accessible to trusted family members.
Schedule a consultation with an elder law attorney. Elder law is a specialized field that covers Medicaid planning, guardianship, estate planning, and long-term care financing. General practice attorneys may not have the specific expertise needed for your parent’s situation. The National Academy of Elder Law Attorneys (NAELA) maintains a searchable directory.
Review Medicare and insurance coverage. Understand what your parent’s current plan covers — and what it does not. Medicare does not cover long-term custodial care, for example, but may cover skilled nursing care after a hospital stay. If your parent has a Medigap or Medicare Advantage plan, the coverage rules differ. Our guide to hidden funding sources provides a detailed breakdown of Medicare, VA benefits, life insurance conversions, and grant programs that many families overlook.
Initiate a conversation about finances. This is often the most difficult conversation of the entire caregiving journey. Approach it as a partnership: “Mom, I want to make sure your wishes are followed. Can we look at your accounts together so I understand how things are set up?” If your parent is resistant, an elder law attorney can sometimes facilitate the conversation in a neutral setting.
The statistic that nearly half (47%) of caregivers receive no formal support underscores why proactive legal planning matters. Without legal authority, you cannot access the support systems that exist — you cannot talk to your parent’s doctor, manage their insurance claims, or make decisions about their care. Week 2 is about removing those barriers before you need them.
Stage 3 (Days 15–21): Build the Care Team
By the end of Week 2, you know what your parent needs (Stage 1) and you have the legal authority to act (Stage 2). Week 3 is about assembling the people and organizations who will help you deliver that care. No single person — not you, not a sibling, not a doctor — can manage the full scope of an aging parent’s needs alone. The evidence is clear: 88% of caregivers say they need more help, and those who try to go it alone are at significantly higher risk for burnout and adverse health outcomes.
An effective care team distributes responsibility across multiple roles, reducing the burden on any single person.
The care team should include the following roles. Not every role will be needed in every situation, but each should be considered.
Core members of a coordinated care team and how to engage each one during Week 3.
Team Member
Role
How to Engage
Primary care physician
Medical oversight and coordination; geriatric assessment
Schedule a comprehensive geriatric assessment. Ask specifically about fall risk, medication review, and cognitive screening.
Call your local AAA (find it via the Eldercare Locator at 1-800-677-1116). Request a formal in-home needs assessment and information about Medicaid, respite, and nutrition programs.
Geriatric care manager
Professional assessment; care plan development; ongoing coordination
Consider hiring a care manager if you are long-distance or if the situation is complex. The Aging Life Care Association maintains a directory of certified professionals.
Hold a family meeting in Week 3. Assign specific tasks (medical appointments, bill-paying, grocery shopping) based on proximity and availability, not guilt.
Home health agency or in-home care provider
Personal care; homemaking; companionship
If the needs assessment identified ADL deficits, begin researching agencies. Our guide to in-home care services provides a framework for evaluating providers.
If your parent has received a dementia diagnosis, the care team should also include a neurologist or geriatric psychiatrist who specializes in cognitive disorders. Dementia care requires a different coordination model than general aging care because the disease progresses through distinct stages with changing needs. Our stage-by-stage dementia caregiving guide explains what changes at each stage and how to adapt the care plan accordingly.
Sibling coordination deserves special attention during Week 3. The Pew Research Center survey found that women caregivers report more negative impacts than men — 47% of women vs. 30% of men say caregiving has negatively affected their emotional well-being, and 38% vs. 26% report negative impacts on physical health. These disparities often emerge from unequal distribution of caregiving labor within families. A structured family meeting with a written division of responsibilities can prevent resentment from building over time.
Stage 4 (Days 22–30): Implement Respite, Support, and Self-Care Scaffolding
The first three weeks of caregiving are almost entirely outward-facing: assessing your parent’s needs, securing legal authority, building a team. Week 4 is the week you turn inward — not because your parent’s needs have been solved, but because the single greatest predictor of whether you can sustain caregiving over the long term is whether you build your own support system now, before burnout has a chance to take hold.
The research on caregiver burden is unambiguous about what matters most. A systematic review by van der Lee and colleagues (2014), published in the International Journal of Geriatric Psychiatry and cited in the Schulz and Beach (2020) Annual Review, found that care recipient behavioral symptoms — agitation, irritability, combativeness, repetitive questioning — are stronger predictors of caregiver burden and depression than cognitive decline or functional status. In other words, the emotional and behavioral challenges of caregiving are more draining than the physical tasks. This means that emotional support is not a luxury; it is a structural necessity of sustainable caregiving.
Week 4 has three priorities:
Enroll in a caregiver support group. The SeniorLiving.org survey found that 62% of caregivers agree with the statement: “I wish I could talk to other caregivers who understand what I’m going through.” Support groups — whether in-person through your local AAA or online through organizations like the Caregiver Action Network — provide validation, practical tips, and a space to express feelings that family members may not understand. The evidence from the Schulz and Beach review suggests that multicomponent interventions addressing both the practical and emotional dimensions of caregiving are the most effective.
Explore respite care options. Respite care is temporary relief for the primary caregiver. Options include: adult day care centers (structured programs during daytime hours), in-home respite (a home health aide or volunteer stays with your parent for a few hours), and short-term residential respite (a nursing home or assisted living facility provides care for a week or two). Our article on adult day care for caregiver respite explains how day programs support both your health and your parent’s social engagement.
Establish a basic self-care baseline. This does not mean a spa day or a meditation retreat. It means: one 20-minute block of uninterrupted time per day that is yours; one full night of sleep per week without caregiving interruptions (arranged through respite or a sibling); one meal per day that you eat sitting down, not standing over the kitchen counter. These are not aspirational goals. They are minimum viable self-care standards.
By the end of Day 30, you should have: a support group meeting on your calendar, at least one respite option identified (even if not yet used), and a self-care baseline that you have actually practiced for at least three days. These are the scaffolding that will carry you through the months ahead.
What a Sustainable Care Rhythm Looks Like After 90 Days
The first 30 days are about stabilization. By Day 90, the goal is a sustainable rhythm — a pattern of care that does not require constant crisis management and that preserves your own health alongside your parent’s. A sustainable care rhythm typically includes the following elements:
A regular check-in schedule with the care team. The primary care physician is seen every three to six months. The care manager (if you have one) is contacted monthly. Siblings have a standing 30-minute video call every two weeks to review what is working and what is not.
A shared family communication system. Whether it is a group chat, a shared document, or a care coordination app, the system captures medication changes, doctor’s notes, and upcoming appointments in one place that everyone can access.
A recurring respite plan. Respite is not a one-time emergency measure. It is a scheduled part of the care calendar — every Tuesday afternoon, or the first weekend of every month, or whatever pattern fits your situation. The National Institute on Aging emphasizes that regular respite is essential for preventing caregiver burnout.
A personal self-care baseline that has become routine. The 20-minute daily block is now non-negotiable. The support group is a regular commitment. You have identified at least one activity — walking, reading, cooking, gardening — that is yours and that you protect from caregiving encroachment.
Not every caregiving journey will reach this rhythm. Some situations — a rapidly progressing dementia, a parent with complex medical needs, a family that cannot or will not share responsibility — require more intensive intervention. If your assessment in Stage 1 reveals needs that exceed what can be managed at home, or if the care team you build in Stage 3 identifies the need for a higher level of care, our long-term care decision framework provides a structured approach to evaluating assisted living, nursing home, and memory care options.
The four-stage framework outlined here is not a guarantee that caregiving will be easy. It is a guarantee that you will not have to face the first month without a map. The evidence is clear: structured entry into caregiving — assessment first, legal infrastructure second, team third, self-care fourth — reduces the risks of burnout, family conflict, and missed needs that plague unstructured caregiving. You do not have to do this alone, and you do not have to do it all at once. One week at a time.


Comments
Join the discussion with an anonymous comment.