Live-In Caregiver for a Parent with Dementia: A Complete Guide to Hiring, Training, and Safety at Every Stage
stage guideearly, middle, late stagesundowning, wandering, agitation, repetitive questioningReviewed: 2026-06-19
Live-In Caregiver for a Parent with Dementia: A Complete Guide to Hiring, Training, and Safety at Every Stage
By Editorial Team
dementia live-in care
hiring a caregiver
dementia safety
memory care costs
Alzheimer's care
Why Dementia Changes the Live-In Care Equation
Hiring a live-in caregiver for a parent with Alzheimer's or another form of dementia is not the same as hiring one for an older adult who simply needs help with mobility or housekeeping. The difference is not subtle — it is structural. Dementia changes how a person perceives their environment, communicates, and regulates their emotions. A caregiver who is excellent at assisting with bathing and meal preparation may be entirely unprepared for the behavioral challenges that come with middle-stage dementia, such as sundowning, repetitive questioning, or attempts to leave the house at 2 a.m.
Families often underestimate this intensity. The result is rapid caregiver turnover — a live-in caregiver quits after a few weeks because they cannot manage the sleep disruption or the emotional toll — and the family is left scrambling for a replacement or facing an unplanned move to memory care. This guide is written for adult children and spousal caregivers who are considering live-in care as an alternative to facility placement. It focuses specifically on the hiring, training, and safety management of a professional live-in caregiver for a person with dementia, not on family-led care at home. If you are looking for guidance on managing dementia behaviors yourself, our Dementia Care at Home guide covers that territory.
How Dementia Live-In Care Differs from Standard Live-In Care
In a standard live-in arrangement, a caregiver works a 24-hour shift that includes eight hours of uninterrupted sleep, plus meal and rest breaks. The caregiver is present to assist with activities of daily living — bathing, dressing, toileting, meal preparation — and to provide companionship and safety oversight. The caregiver can reasonably expect to sleep through the night most nights.
Dementia changes that equation in several fundamental ways.
Sleep interruption is the norm, not the exception. Sundowning — the increase in confusion, agitation, and restlessness that occurs in the late afternoon and evening — often extends into the night. A person with dementia may wake repeatedly, try to get out of bed, or become convinced it is time to get dressed and start the day. The live-in caregiver's sleep is fragmented, which is physically unsustainable over weeks and months.
Wandering risk requires constant vigilance. A person with dementia may attempt to leave the house at any hour, often with a specific but false purpose — "I need to go to work," "I have to pick up the children from school." The caregiver cannot simply lock the door and go back to sleep. They must redirect, reassure, and monitor. Our guide on sundowning and nighttime safety provides deeper strategies that every live-in caregiver should be trained to use.
Communication and behavior management skills are essential. A standard caregiver may not know how to respond to repetitive questioning, paranoia, or aggression. A dementia-trained caregiver must be able to redirect without arguing, validate without reinforcing false beliefs, and de-escalate agitation without physical restraint. These are learned skills, not innate traits.
The caregiver's role changes as the disease progresses. What works in the early stage — medication reminders, light supervision, companionship — becomes inadequate in the middle stage, when full assistance with ADLs, wandering prevention, and behavior redirection are needed. By the late stage, the caregiver is providing total care: feeding, incontinence management, and 24/7 monitoring. The family must be prepared to adjust the caregiver's responsibilities — or replace the caregiver — as the disease advances.
What a Live-In Caregiver Handles at Each Dementia Stage
One of the most common mistakes families make is hiring a caregiver based on the person's current needs without anticipating how those needs will change. Dementia is a progressive disease, and the care requirements at each stage are dramatically different. The table below outlines what a live-in caregiver should be prepared to handle at each stage, along with the skills and training required.
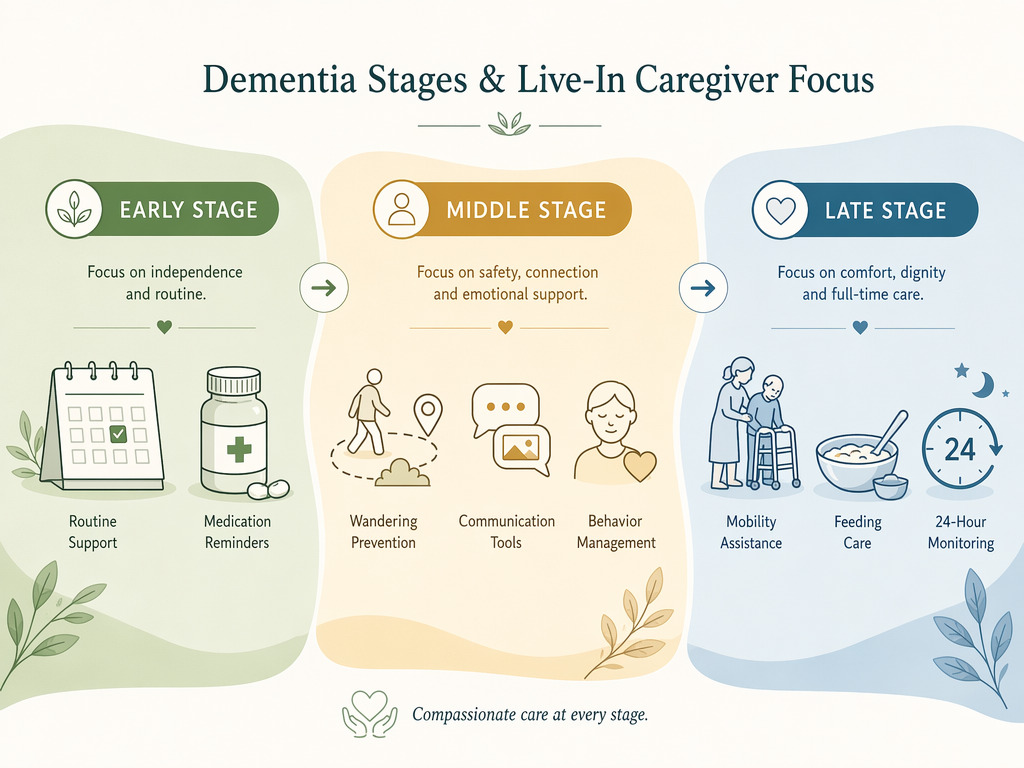
Dementia progression stages and the corresponding care focus for a live-in caregiver.
Stage-by-stage care expectations for a live-in caregiver supporting a person with dementia. Active care hours are estimates and vary by individual.
10–16 hours of active care; sleep is frequently interrupted
Late
Total mobility assistance, feeding, incontinence care, 24/7 monitoring, end-of-life comfort
Full personal care, feeding techniques, skin care, palliative care awareness, ability to work in shifts or with backup
24/7 active care or near-constant monitoring; single caregiver is often insufficient
For a detailed look at what late-stage care involves, see our Late-Stage Alzheimer's Care Guide. It covers the daily care routines that a live-in caregiver will need to manage, including feeding, positioning, and skin integrity.
Key Interview Questions for a Dementia-Specific Live-In Caregiver
Standard caregiver interview questions — "Why are you interested in this position?" or "What experience do you have?" — will not tell you whether a candidate can handle dementia-specific challenges. You need scenario-based questions that reveal how the candidate thinks, reacts, and communicates under the conditions they will actually face.
The Family Caregiver Alliance recommends asking candidates to describe specific experiences with memory problems, transfers, and difficult behaviors. Below is a set of dementia-specific questions that go beyond the standard screening.
"Tell me about a time a client with dementia became agitated or aggressive. What did you do?" Look for answers that describe de-escalation without physical restraint, redirection, and a calm tone. Red flags: "I just let them calm down on their own" or "I called the family."
"How do you handle sundowning? What strategies have you used to reduce evening confusion?" A strong answer will mention increasing daytime activity, reducing late-afternoon caffeine, turning on lights before sunset to minimize shadows, and maintaining a consistent evening routine.
"What would you do if my parent tried to leave the house at 2 a.m.?" The right answer involves gentle redirection, not confrontation. The caregiver should explain how they would validate the person's concern ("I understand you need to go to work, but it's still nighttime — let's sit down and have a cup of tea first") and then guide them back to bed.
"Describe your experience with repetitive questioning. How do you respond when a client asks the same question every few minutes?" Look for answers that involve distraction (offering a snack, a familiar activity, or a change of scenery) rather than reminding the person that they already asked.
"How do you approach bathing or toileting with a person who is resistant or confused?" The candidate should describe maintaining the person's past routine, using a calm and reassuring tone, and never leaving the person unattended. They should also be aware of safety features like grab bars and shower chairs.
Home Modifications for Dementia Safety
A live-in caregiver cannot do their job safely if the home itself is not set up for dementia care. Standard senior safety upgrades — grab bars, non-slip flooring, adequate lighting — are necessary but not sufficient. Dementia-specific modifications address the behaviors that put a person at risk: wandering, cooking accidents, and confusion triggered by shadows or reflections.
Families often fail to budget for these modifications. According to the 2026 A Place for Mom cost data, home safety modifications for dementia can add $2,000 to $15,000 or more to the total cost of in-home care. The table below lists the most critical dementia-specific modifications and their estimated cost ranges.
Essential dementia safety modifications: alarmed doors for wandering prevention and stove auto-shutoff devices for kitchen safety.
Dementia-specific home safety modifications with estimated cost ranges. Costs are national medians and may vary by region and contractor.
Modification
Purpose
Estimated Cost Range
Notes
Alarmed doors and windows
Alert the caregiver when the person attempts to leave
$200 – $1,500
Motion-sensor alarms or magnetic contact alarms; some systems can send alerts to the caregiver's phone
Stove auto-shutoff device
Prevent cooking fires if the person turns on the stove and forgets
$250 – $1,500
Devices that shut off the gas or electric supply after a set period of inactivity or when motion is not detected nearby
Motion-activated night lights
Reduce shadows and confusion during nighttime wandering
$50 – $300
Place along hallways, in the bathroom, and near the bedroom; reduces fall risk and sundowning triggers
Grab bars and non-slip flooring
Prevent falls in the bathroom and other high-risk areas
$150 – $1,000
Standard safety upgrades, but essential for dementia care where balance and coordination are declining
Walk-in tub or accessible shower
Reduce bathing resistance and fall risk
$3,000 – $15,000
Larger investment; consider if the person is resistant to bathing or has significant mobility limitations
For detailed guidance on bathroom safety for a person with dementia, see our Bathroom Remodel for Elderly with Dementia guide. It covers how to design a bathroom that is safe without being disorienting.
Cost Comparison: Dementia-Specialized Live-In vs. Memory Care vs. 24/7 Shift Care
The cost of dementia care is a central concern for most families, and the numbers can be overwhelming. The key insight is that full-time in-home dementia care (44 hours per week) and memory care are roughly cost-comparable, while 24/7 shift care is dramatically more expensive. The decision often comes down to the level of supervision required.
Cost comparison of dementia care options using 2026 national median data from A Place for Mom. The dementia-specialized live-in care estimate is a range based on the 2026 APFM data ($34/hr, 44 hrs/week) and the older DementiaCareCentral estimate (~$6,000/month). Actual costs vary by location, agency, and level of care needed.
Care Option
Monthly Cost (2026 National Median)
Annual Cost
Key Considerations
Full-time in-home dementia care (44 hrs/week)
$6,478
$77,732
One caregiver works a set schedule; does not include overnight awake care; suitable for early to middle stages
Memory care facility
$6,690
$80,280
Includes room, board, 24/7 supervision, and dementia-specific programming; may be more cost-effective when 24/7 awake care is needed
24/7 in-home shift care (3 caregivers, 8-hr shifts)
$24,733
$296,796
Around-the-clock awake care; necessary for late-stage wandering, aggression, or medical instability; far more expensive than memory care
Dementia-specialized live-in care (estimated)
$6,000 – $7,500
$72,000 – $90,000
One caregiver lives in, sleeps 8 hours with interruptions; premium for dementia training; cost varies widely by region and agency
The critical cost parity point is this: when a person with dementia requires 24/7 awake supervision — because of late-stage wandering, aggression, or medical instability — memory care at $6,690/month becomes significantly more economical than 24/7 in-home shift care at $24,733/month. For a deeper analysis of when overnight care at home is still feasible versus when it is time to transition to memory care, see our Overnight Dementia Care decision guide.
Medication Management and Professional Boundaries
One of the most common misunderstandings about live-in care is what a caregiver can and cannot do regarding medication. In most states, only licensed nurses can administer medications — that is, physically place a pill in the person's mouth or apply a topical medication. A live-in caregiver, even one with extensive experience, is generally limited to medication reminders and assistance with self-administration.
This distinction matters because dementia progressively impairs a person's ability to manage their own medications. In the early stage, a caregiver may simply need to remind the person to take their pills. By the middle stage, the person may no longer be able to reliably self-administer, and the family needs a system that the caregiver can legally support.
Use a pill organizer. A weekly or daily pill organizer filled by the family or a pharmacist allows the caregiver to hand the correct dose to the person at the right time without needing to handle the medication bottles.
Maintain a medication log. The caregiver should record each dose given, any missed doses, and any observed side effects. This log is essential for the family and the prescribing physician to track the person's response to medications.
Use pharmacy delivery services. Many pharmacies offer automatic refill and delivery, which reduces the burden on the caregiver and ensures that medications are never missed due to a forgotten trip to the pharmacy.
Consult the prescribing physician and pharmacist. The family should discuss the caregiver's role in medication management with the doctor and pharmacist to ensure compliance with state regulations and to establish a clear plan for handling changes in medication.
When Live-In Care Is No Longer Sufficient: Signs It's Time for Memory Care
Live-in care is not a permanent solution for every person with dementia. There comes a point when the demands of care exceed what a single caregiver — no matter how skilled or dedicated — can safely provide. Recognizing this point is not a failure. It is a compassionate, practical decision that protects both the person with dementia and the caregiver.
The following are specific dementia-related triggers that indicate live-in care may no longer be sustainable.
Late-stage wandering that requires 24/7 awake supervision. If the person attempts to leave the house multiple times per night and cannot be redirected, a single live-in caregiver cannot safely manage this while also getting the rest they need. At this point, memory care's 24/7 awake staffing becomes a safety necessity.
Aggression that exceeds a single caregiver's capacity. Physical aggression, severe agitation, or violent outbursts can put both the caregiver and the person with dementia at risk. If the caregiver is being injured or is unable to de-escalate the behavior, it is time to consider a higher level of care.
Rapid weight loss or feeding difficulties. If the person is refusing to eat, has difficulty swallowing, or is losing weight rapidly, they may need the specialized nutritional support and monitoring that a memory care facility can provide.
Caregiver burnout despite professional help. Even with a live-in caregiver, the family caregiver — often an adult child or spouse — may still experience significant stress, anxiety, and burnout. According to the 2026 A Place for Mom caregiver statistics, 70% of dementia caregivers report that caring for someone with dementia is stressful, and 75% feel stressed or anxious at least monthly. If the family caregiver's health is declining, it is a sign that the current arrangement is not working.
Even with a live-in caregiver in place, the family caregiver needs a backup plan. Live-in caregivers get sick, take vacations, and sometimes quit without notice. When that happens, the family caregiver is suddenly back on duty full-time — often with no warning and no support.
A written contract that covers termination and replacement is essential. The AARP caregiver contract checklist recommends including: duration of employment, specified work hours and locations, detailed responsibilities, payment obligations, live-in details, dispute resolution, liability insurance, termination notice, and flexibility for changing care needs.
Beyond the contract, consider the following backup and respite strategies.
Agency backup agreements. If you hire through an agency, ask about their backup caregiver policy. Many agencies guarantee a replacement within 24–48 hours if the primary caregiver is unavailable.
Respite care services. The Alzheimer's Association and state dementia programs often provide respite care vouchers or referrals to short-term respite facilities. These can give the family caregiver a break while ensuring the person with dementia is cared for in a safe environment.
Family and friend backup network. Identify two or three people — family members, close friends, or neighbors — who can step in for a few hours or a day if the live-in caregiver is unavailable. Have them trained on the person's routine and safety protocols in advance.
Caregiver wellbeing support. The family caregiver's own health matters. Our Caregiver Wellbeing section offers resources on recognizing burnout, managing guilt, and finding emotional support. You cannot care for someone else if you are not caring for yourself.
The Alzheimer's Association (alz.org) and the Family Caregiver Alliance (caregiver.org) are excellent resources for finding local respite programs, support groups, and dementia-specific caregiver training. Both organizations offer free or low-cost services that can make the difference between a sustainable live-in arrangement and a crisis.


Comments
Join the discussion with an anonymous comment.