CDC STEADI Fall Prevention Checklist for Home: A Room-by-Room Guide to Fixing What Matters First
Reviewed: 2026-07-05
CDC STEADI Fall Prevention Checklist for Home: A Room-by-Room Guide to Fixing What Matters First
A practical walkthrough of the CDC STEADI 'Check for Safety' checklist, showing family caregivers which rooms to tackle first, how to install safety devices correctly, and how to combine the checklist with the Stay Independent screener for a complete fall risk assessment.
By Editorial Team
new caregiver
experienced caregiver
long-distance caregiving
spousal caregiver
working caregiver
daily routines
medication management
personal hygiene
care coordination
first steps
ADLs
IADLs
If you have one afternoon and the CDC STEADI fall prevention checklist for home open on your phone, do not start by trying to make every room perfect. Start where a fall is most likely to become serious: the bathroom and the stairs. Then move fast through the cheap hazards that do not require debate or a contractor: throw rugs, poor lighting, cords, cluttered walking paths, and anything your parent steps around every day without noticing.
The CDC’s “Check for Safety” brochure is the right starting document because it is free, non-commercial, and built as a room-by-room home walkthrough for older adults and caregivers. It appears on the CDC STEADI Patient and Caregiver Resources page, alongside other fall prevention materials for families.[1] This article is a companion for using that checklist well. The official CDC PDF is still the document to open, print, or save before you walk the house.
The urgency is not theoretical. More than 1 in 4 adults age 65 and older falls each year, and falls are the leading cause of fatal and nonfatal injury in that age group.[1] The newer AGS STEADI update cites approximately $80 billion in annual nonfatal fall medical costs, using 2020 data.[2] More than 75% of falls happen in or near the home.[1] That is why the ordinary house deserves a more serious look than “be careful” and a more useful plan than “remove hazards.”
Before You Walk the House, Decide What Counts as First
A checklist treats each item as a box. A caregiver has to treat each item as a decision: fix today, schedule soon, or hand off because a bad fix could make things worse.
Walk the home in daylight first, then repeat the main nighttime route with lights off or dimmed the way your parent actually uses the house. Bring painter’s tape, a pen, your phone camera, and the CDC checklist. Tape does not fix the hazard; it keeps everyone from pretending later that the loose rug, dark landing, or missing handrail was vague.
Priority
What goes here
What to do
Fix today
Loose throw rugs, cluttered walking paths, cords across routes, poor night lighting, items stored too high or too low
Remove, relocate, tape temporarily only if removal is not possible, add lighting, clear the path
Measure, choose proper hardware, and decide whether the job needs a professional
Hand off
Anything load-bearing, structural, electrical, uncertain, or likely to fail if installed badly
Call an OT, CAPS specialist, or contractor instead of improvising
This order helps when family resistance shows up. A parent may argue that the kitchen is fine, the rug has always been there, or the bathroom does not need “hospital equipment.” You do not have to win every argument at once. Remove what is obviously unsafe, document what needs skilled work, and save the hardest conversations for the places where the consequence of a fall is highest.
Bathroom: The Room Where “Install Grab Bars” Is Not Enough
Bathrooms deserve the first slow pass. Water, soap, tile, turning, stepping over tub walls, and standing from the toilet all combine in a small space. The CDC checklist includes the bathroom as one of its room-by-room safety areas, and the NIA’s room-by-room fall prevention guidance also emphasizes bathroom fixes such as grab bars and non-slip surfaces.[1][3]
Start by watching the movements, not the decor. Where does your parent place a hand when getting into the shower? What do they grab when standing from the toilet? Do they step onto a loose bath mat? Is shampoo stored where reaching requires twisting? Is there a clear place to sit if standing in the shower is getting difficult?
Then separate the quick fixes from the serious installations.
Remove loose bath mats or replace them with safer non-slip options that do not bunch, slide, or curl at the corners.
Move soap, shampoo, towels, and clean clothing within easy reach so bathing does not require stretching or turning on a wet surface.
Add brighter lighting if the bathroom is dim at night, especially between the bedroom and toilet.
Use a shower chair or tub bench when standing balance is no longer reliable, but make sure it fits the bathing setup and does not create a new trip point.
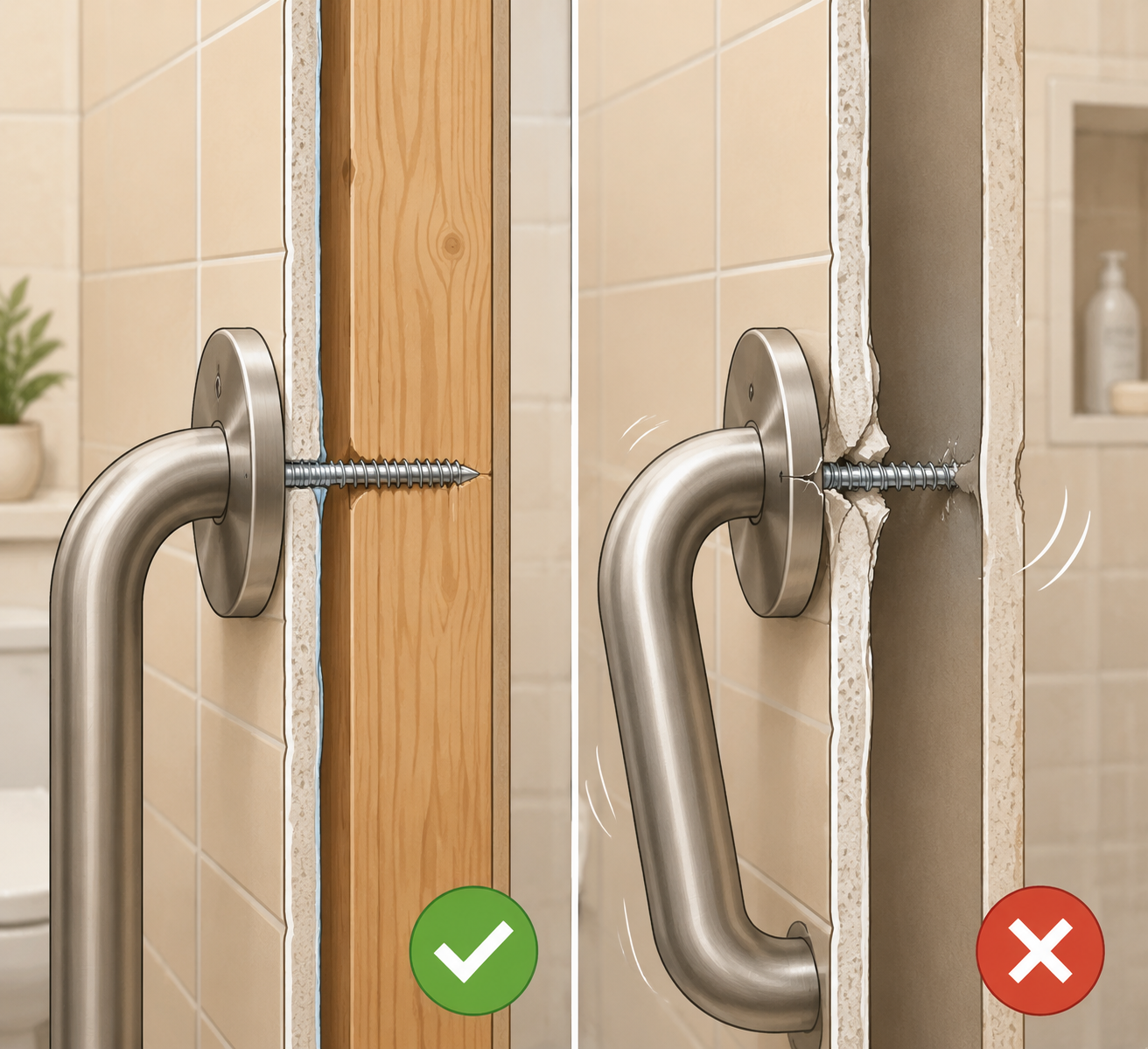
Install grab bars only when they can be secured properly; do not count towel bars, suction handles, or drywall-only anchors as fall protection.
The grab bar point is where many home safety lists become too polite. A towel bar is not designed to hold a falling body. A grab bar must be anchored into wall studs or another appropriate structural backing, not just into drywall.[3] If you cannot identify the studs, do not know what is behind the wall, or are dealing with tile, fiberglass, old plaster, or an unusual shower surround, that is not the moment for confidence based on a hardware-store package.
Stairs are the other place to slow down. The question is not only whether the stairs look neat. It is whether your parent has a reliable handhold, enough light to see each tread edge, and a route that still works when they are tired, carrying laundry, or waking up at night.
Use the CDC checklist as the visual prompt, then inspect the stair route in four passes: the treads, the handrails, the lighting, and the landings. If any pass fails, put the stairs near the top of the action list rather than burying them under easier chores.
Treads: remove loose objects, repair curled carpet edges, and check whether tread surfaces are slippery or uneven.
Handrails: make sure there is a secure rail where the person actually needs support, not just a decorative rail that stops too soon.
Lighting: check both the top and bottom of the stairs, and make sure switches are reachable before stepping onto the stairs.
Landings: clear shoes, baskets, pet items, and packages from the places where someone turns or regains balance.
A burned-out bulb is a Saturday fix. A missing handrail, loose railing, uneven stair, electrical change, or failing tread is not the place to improvise. If the work needs to bear weight, alter wiring, or correct a structural problem, hand it to the right professional. Families comparing an occupational therapist, CAPS specialist, and contractor can use this guide to choosing the right home modification professional before hiring.
Floors and Walking Paths: Fix the Cheap Hazards Before Anyone Votes on Them
Floors are where families often lose momentum because the hazards look small. A rug edge is not dramatic. A phone cord across a hallway does not feel like a medical issue. A stack of magazines beside a favorite chair may have been there for years. Still, these are exactly the hazards to remove quickly because the fix is usually cheap and the negotiation should be short.
Walk every usual route: front door to chair, chair to bathroom, bedroom to bathroom, kitchen to table, laundry route, and any path to a pet bowl, thermostat, or mailbox. Mark anything that forces a sidestep, shuffle, reach, or turn. Then fix what can be fixed without waiting for a larger project.
Remove throw rugs, especially on routes used at night or while carrying something.
Move cords out of walking paths instead of taping them across the floor as a permanent solution.
Clear low tables, baskets, shoes, and pet items from narrow routes.
Check thresholds between rooms for raised edges that catch toes or mobility aids.
Improve lighting on any path used after dark, especially the bedroom-to-bathroom route.
A bedroom can look safe in daylight and still be a fall setup at night. The important route is usually bed to bathroom, bed to light switch, and bed to phone. Walk it in the conditions your parent actually uses: slippers on, glasses off, half awake, maybe trying not to wake anyone.
Put a lamp, phone, glasses, and any needed mobility aid within easy reach of the bed.
Add nightlights along the bathroom route, not just inside the bedroom.
Remove bedding, cords, shoes, and storage bins from the floor beside the bed.
Check whether the bed height makes standing difficult or causes feet to dangle.
Escalate if getting in and out of bed has become a transfer problem rather than a housekeeping problem. That may call for an occupational therapist’s assessment instead of another rearrangement of the nightstand.
Kitchen: Reduce Reaching, Carrying, and Turning
The kitchen usually produces a different kind of fall risk: reaching overhead, bending low, turning quickly, and carrying hot or heavy items while stepping around obstacles. The fix is less about remodeling and more about moving the daily-use items into the right zone.
Move everyday dishes, mugs, pans, and food items to shelves between shoulder and knee height.
Remove small rugs near the sink, stove, and refrigerator unless they are truly stable and low-profile.
Clear the route between refrigerator, sink, stove, and table.
Make sure spills can be cleaned without rushing across the room for towels or supplies.
Be careful with “helpful” storage changes that make the room tidy but less usable. If the coffee mug moves to a high cabinet because it looks better there, you have not reduced risk. You have hidden it.
Outdoor Areas: Treat the First and Last Ten Feet Seriously
The CDC checklist includes outdoor areas because home fall risk does not stop at the door.[1] For many older adults, the most important outdoor zone is the first and last ten feet: porch, threshold, steps, walkway, mailbox route, driveway edge, and the place where packages land.
Check for uneven walkway sections, loose bricks, cracked steps, and raised thresholds.
Add or improve lighting at entrances used after dark.
Keep packages, hoses, planters, and seasonal decorations out of the walking route.
Make sure railings at outdoor steps are secure enough to use, not just present.
Outdoor repairs often cross the line into contractor work faster than indoor decluttering does. A loose mat can leave today. A broken step, failed railing, or uneven walkway needs proper repair, not a warning taped to the door.
What the Home Walkthrough Cannot See
A clean, well-lit house does not prove someone is at low fall risk. The CDC STEADI framework includes screening and clinical follow-up because fall risk also lives in balance, strength, vision, medications, blood pressure changes, fear of falling, and the history your parent may not volunteer while you are looking at rugs.[4]
The AGS 2024 workgroup update recommends starting with three STEADI screening questions before using the full 12-item Stay Independent questionnaire: “Have you fallen?”, “Do you feel unsteady?”, and “Are you worried about falling?”[2] Those questions are short enough to ask at the kitchen table after the walkthrough, and they catch the part of the problem the house cannot answer.
If the answer to any of those questions is yes, or if the Stay Independent screener raises concern, the next step is not another lamp. It is a broader fall-risk conversation with a clinician. That conversation may include medication review, vision, strength and balance, blood pressure, footwear, assistive devices, and whether physical or occupational therapy is appropriate. For the medication piece, use a caregiver’s guide to medication review for fall prevention as a preparation tool, not as a reason to change medicines on your own.
This is also where family resistance can change shape. A parent who objects to “safety-proofing” may respond differently to three questions from a CDC-backed fall prevention framework than to an adult child pointing at the rug again. If the resistance started after a hospitalization or recent fall, the guide on why parents resist fall prevention after the hospital may be the more useful handoff than another checklist.
Turning the CDC Checklist Into an Action Plan
After the walkthrough, do not leave the CDC checklist as a marked-up document with twenty equal problems. Convert it into a short work order.
Open the official CDC “Check for Safety” brochure from the STEADI Patient and Caregiver Resources page.
Walk the bathroom and stairs first, marking anything that affects wet surfaces, transfers, handholds, lighting, treads, or railings.
Remove low-cost hazards the same day: throw rugs, clutter, cords, poor night lighting, and badly placed daily-use items.
Do not install grab bars into drywall alone, and do not treat towel bars as grab bars.
Hand off structural, electrical, load-bearing, or uncertain work to an OT, CAPS specialist, or qualified contractor.
Ask the Three Key Questions and use the Stay Independent screener to decide whether the home audit should become a clinical fall-risk conversation.
The CDC checklist earns its keep when it changes what happens next: bathroom and stairs first, cheap hazards removed now, grab bars installed correctly or not at all, and the visual walkthrough paired with STEADI screening questions that catch the risks no flashlight can show.

Comments
Join the discussion with an anonymous comment.