Overnight Care Decision Framework: Matching Care Models to Nighttime Risk Profiles
A structured guide for adult children deciding which overnight care model fits their parent's specific nighttime risks — falls, wandering, sundowning, or incontinence — with cost anchors, a matching matrix, and a step-by-step decision flowchart to avoid overpaying or under-protecting.
By Editorial Team
overnight care
nighttime care
sleeping shift
awake shift
live-in care
24-hour care
care coordination
cost comparison
📄
A printable version of this guide is available. Use your browser's print function (Ctrl+P / ⌘P) to save or print.
Why "Overnight Care" Means Different Things — and Why It Matters
When a family first starts talking about overnight care, the phrase sounds straightforward: someone stays with Mom or Dad through the night. But in practice, "overnight care" covers four fundamentally different arrangements, and the difference between them is measured in thousands of dollars per month and, more importantly, in whether your parent actually gets the support they need.
The core mistake families make is treating overnight care as a single product. They call an agency and ask for "nighttime help" without understanding whether they need a caregiver who sleeps on the premises and wakes when called, or one who stays alert through the entire shift. The wrong choice means either paying for alert coverage you do not need or — far worse — hiring a sleeping caregiver for a parent who needs active monitoring.
The Four Overnight Care Models
Four overnight care models with cost anchors based on 2025–2026 national median data from CareScout, SeniorSite, and CareYaya. Actual costs vary by region and agency.
Model
How It Works
Typical Cost Anchor
Best For
Sleeping Shift
Caregiver sleeps at the home, available if needed. Usually 8–12 hours. Not expected to stay awake.
~$200/night flat rate ($120–$200 range)
Low-risk nights with predictable, infrequent needs
Awake Shift
Caregiver stays awake and alert for the entire shift. Provides active monitoring and assistance.
~$250+/night or $25–$35/hour
Frequent toileting, wandering risk, severe sundowning, high fall risk
Live-In
Caregiver lives in the home, provides up to 16 hours of care per day with 6–8 hours of uninterrupted sleep.
$200–$350/day flat rate
Moderate needs that span day and night but allow caregiver downtime
24/7 Rotating
Two or three caregivers working 8- or 12-hour shifts, paid hourly plus overtime.
If you are unsure whether your parent needs overnight care at all, start with our red flags guide — then use this framework to match the right model to your parent's specific nighttime risk profile.
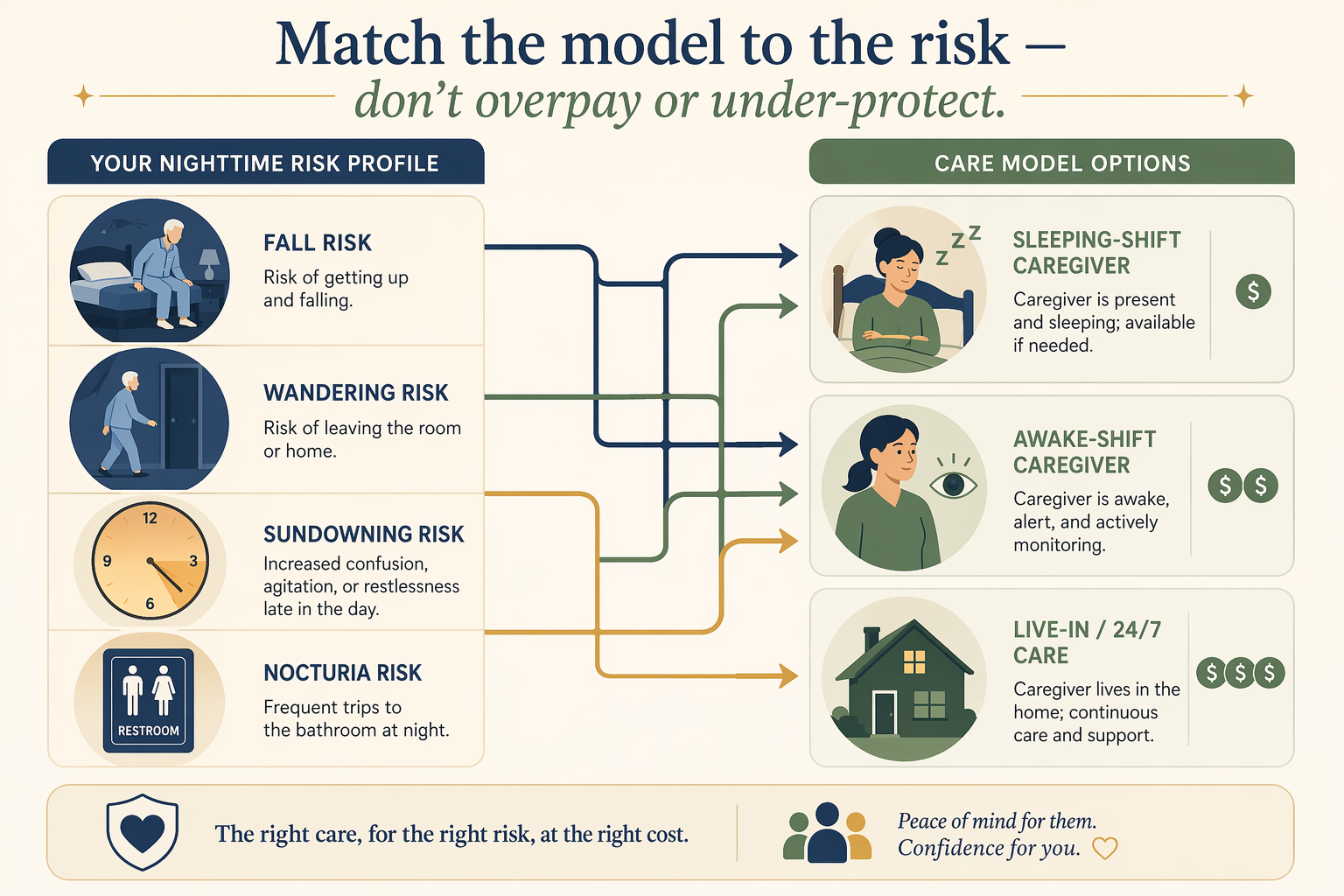
Match the model to the risk — don't overpay or under-protect.
The Four Nighttime Risk Profiles That Determine the Right Model
The right overnight care model depends entirely on what happens between bedtime and morning. Sleep problems affect 40% to 70% of seniors, according to SeniorSite, and many cases go undiagnosed. But the specific type of nighttime disruption determines whether a sleeping caregiver is sufficient or an awake caregiver is essential.
Risk Profile 1: Falls Risk and Nocturia
Nocturia — waking up two or more times per night to urinate — is the single most common driver of overnight falls. A University of Alabama at Birmingham study found that seniors with nocturia are nearly 30% more likely to fall, and 76.8% of older adults with hip fractures reported at least one nocturnal void. The National Institutes of Health notes that most falls occur overnight and that evening falls tend to result in more serious injuries than daytime falls.
For this profile, the key question is frequency. A parent who gets up once or twice per night and can safely navigate the bed-to-bathroom route may only need a sleeping caregiver who can assist if called. But a parent who gets up four or more times, has unsteady gait, or has already fallen at night likely needs an awake caregiver who can intervene before a fall happens.
Risk Profile 2: Wandering and Elopement
Wandering is one of the most dangerous dementia-related behaviors, and it is most dangerous at night. The Alzheimer's Association reports that 6 in 10 people with dementia will wander at least once, and many do so repeatedly. Nearly half of seniors who wander will suffer an injury or worse if not found within 24 hours.
A sleeping caregiver is not appropriate for this risk profile. Wandering can happen silently and quickly — a person with dementia may get dressed, open a door, and walk outside without making a sound. Only an awake caregiver who is actively monitoring can respond in time. Families managing this risk should also develop a comprehensive wandering safety plan that goes beyond overnight care.
Risk Profile 3: Sundowning and Agitation
Sundowning refers to increased confusion, anxiety, and agitation that begins in the late afternoon and extends into the night. The Mayo Clinic notes that it affects 20% to 45% of people with Alzheimer's, manifesting as pacing, aggression, ignoring directions, and difficulty separating reality from dreams. The Alzheimer's Association adds that factors like fatigue, low lighting, and disruption of the body's internal clock can worsen symptoms.
Sundowning creates a unique overnight care challenge because the peak of confusion often coincides with the time when family caregivers are most exhausted. A sleeping caregiver cannot manage active agitation or reorientation needs. Families dealing with moderate to severe sundowning typically need an awake caregiver who can provide reassurance, maintain a calm environment, and prevent escalation.
Risk Profile 4: Incontinence and Repositioning Needs
Frequent incontinence episodes or the need for repositioning to prevent pressure ulcers creates a high-interruption night. A caregiver may be needed every one to two hours for toileting, changing, or turning. At this frequency, a sleeping caregiver cannot get the five hours of uninterrupted sleep that federal rules require for sleep-time pay exclusions to apply. If interruptions prevent five hours of sleep, the entire shift becomes billable at the awake rate.
This profile often signals that overnight care alone may not be sufficient. When a parent needs repositioning or toileting assistance every one to two hours around the clock, the family should evaluate whether a live-in or 24/7 rotating model is more appropriate.
Risk-Profile-to-Care-Model Matching Matrix
The following matrix maps each risk profile to the most appropriate care model. Use it as a starting point, then refine based on your parent's specific frequency and severity.
Risk-profile-to-care-model matching matrix.
Matching matrix: "Best match" indicates the most cost-effective and appropriate model. "Possible" means it may work with adjustments. "Not appropriate" means the model cannot safely meet the need.
Risk Profile
Sleeping Shift
Awake Shift
Live-In
24/7 Rotating
Falls / Nocturia (1–2x/night)
Best match
Possible
Overkill
Overkill
Falls / Nocturia (3+ times/night)
Not appropriate
Best match
Possible
Possible
Wandering / Elopement
Not appropriate
Best match
Possible
Best match if daytime wandering also present
Sundowning / Agitation (mild)
Possible
Best match
Possible
Overkill
Sundowning / Agitation (severe)
Not appropriate
Best match
Possible
Best match if daytime agitation also present
Incontinence / Repositioning (frequent)
Not appropriate
Possible
Best match
Best match if round-the-clock needs
Decision Flowchart: Is Your Parent Safe Alone for 6+ Hours at Night?
Use this step-by-step self-assessment to determine which care model fits your situation. Answer each question honestly — the goal is to match the model to the risk, not to minimize cost at the expense of safety.
Decision flowchart for matching overnight care model to risk profile.
Step 1: Can your parent get through the night without needing help to use the bathroom, reposition, or take medication? If YES, proceed to Step 2. If NO, count the average number of nighttime interruptions.
Step 2: Has your parent fallen in the past 12 months? A history of a single fall doubles the chances of falling again, per the CDC STEADI initiative. If YES and the fall occurred at night, proceed to awake shift evaluation.
Step 3: Does your parent have a dementia diagnosis? If YES, assess wandering risk. Has your parent attempted to leave the home at night, or expressed a desire to "go home" or "go to work" after dark? If YES, an awake shift is the minimum safe option.
Step 4: Does your parent experience sundowning? If confusion, anxiety, or agitation begins in the late afternoon and extends into the night, evaluate severity. Mild sundowning (brief confusion that resolves with reassurance) may be manageable with a sleeping caregiver. Moderate to severe sundowning (pacing, aggression, inability to settle) requires an awake caregiver.
Step 5: How many hours of uninterrupted sleep do you, the family caregiver, get per night? If you are waking up three or more times per night to assist your parent, you are sleep-deprived. A study found that 70% of dementia family caregivers ultimately placed their loved one in a nursing home primarily because of sleep disruptions and exhaustion from overnight caregiving (Rowe et al., Alzheimer's & Dementia Journal). Your sleep matters — and it is a valid reason to bring in overnight help.
Cost Comparison: Sleeping Shift vs. Awake Shift vs. Live-In vs. 24/7 Rotating
Cost is often the deciding factor, but the cheapest option is only a bargain if it actually meets the need. The table below projects monthly costs for each model based on national median data. Regional variation is significant — for example, Minnesota averages $43/hour while Mississippi averages $24/hour, according to SeniorLiving.org.
Monthly cost comparison of overnight care models (national median estimates, 2025–2026).
Monthly cost projections based on 2025–2026 national median data from CareScout, SeniorSite, CareYaya, and SeniorLiving.org. Actual costs vary by region, agency, and level of need.
Model
Typical Rate
Monthly Estimate (30 days)
Best For
Sleeping Shift
$120–$200/night flat
$3,600–$6,000
Low-risk, low-interruption nights
Awake Shift
$250+/night or $25–$35/hr
$7,500–$10,500+
Frequent needs, wandering, sundowning
Live-In
$200–$350/day flat
$6,000–$10,500
Moderate day-and-night needs with caregiver downtime
Hiring Pathway: Agency vs. Private Hire for Overnight Care
Once you have identified the right care model, the next decision is how to hire. You have two main pathways: work with an agency or hire a private caregiver directly. Each has trade-offs that go beyond the hourly rate.
Agency Hire
Costs 20–30% more than private hire, according to SeniorLiving.org
Provides backup coverage if the assigned caregiver calls out sick
Handles payroll taxes, workers' compensation insurance, and compliance with labor laws
Screens and trains caregivers; typically bonds and insures them
Easier to replace a caregiver who is not a good fit
Private Hire
Lower cost — you pay the caregiver directly, typically $15–$25/hour depending on your market
You become the employer, responsible for payroll taxes, workers' comp, and compliance with federal and state labor laws
No backup coverage — if the caregiver cannot make it, you are on your own
You handle vetting, background checks, and references yourself
More flexibility in scheduling and care arrangements
When to Reassess: The Sliding Scale from Occasional Nights to 24/7 Care
Overnight care needs are rarely static. A parent who needs a sleeping shift twice a week today may need an awake shift every night in six months. The key is to recognize the signals that indicate it is time to move up the care ladder.
Signal 1: Your parent's nighttime interruptions increase in frequency or severity. If they go from one to two bathroom trips per night to four or more, or if they begin getting out of bed without calling for help, the risk profile has shifted.
Signal 2: A fall occurs at night, even if no serious injury results. A single fall doubles the risk of another fall, and nighttime falls tend to cause more serious injuries than daytime falls.
Signal 3: Wandering behavior emerges or escalates. If a parent who previously stayed in bed at night begins attempting to leave the home, immediate escalation to awake care is necessary.
Signal 4: The family caregiver's sleep deprivation reaches a crisis point. More than 60% of caregivers experience symptoms of burnout, according to the Cleveland Clinic, and sleep disruption is a primary driver. If you are consistently getting fewer than five hours of sleep per night, you cannot sustain caregiving long-term.
Signal 5: Daytime needs escalate alongside nighttime needs. When a parent requires assistance with multiple activities of daily living during the day and also needs frequent nighttime attention, a live-in or 24/7 rotating model may be more cost-effective than separate day and night caregivers.
When overnight care alone is no longer sufficient, our 24-hour home care decision framework can help you evaluate whether it is time to move to round-the-clock coverage.




Comments
Join the discussion with an anonymous comment.