Choosing among senior care options can feel overwhelming after a dementia diagnosis. This guide uses the ADL and IADL framework to map care levels to functional decline, helping families understand when memory care becomes the necessary next step.
By Editorial Team
early-stage Alzheimer's
middle-stage Alzheimer's
late-stage Alzheimer's
wandering
sundowning
agitation
repetitive questioning
sleep disturbances
eating refusal
dementia communication
safety planning
hospice and end-of-life
BPSD
The search for senior care options usually starts too politely. A parent has a diagnosis. Everyone agrees they need “a little help.” Then the evidence gets harder to explain away: the pillbox is wrong again, the refrigerator is full but meals are not happening, a utility bill is unpaid, the stove was left on, or a spouse admits they are afraid to sleep through the night.
At that point, the useful question is not “Which facility is best?” It is “What can my parent still do safely, what has already broken down, and who is responsible when it breaks down again?” Dementia care decisions become clearer when families stop treating care as a menu and start treating it as a progression tied to function.
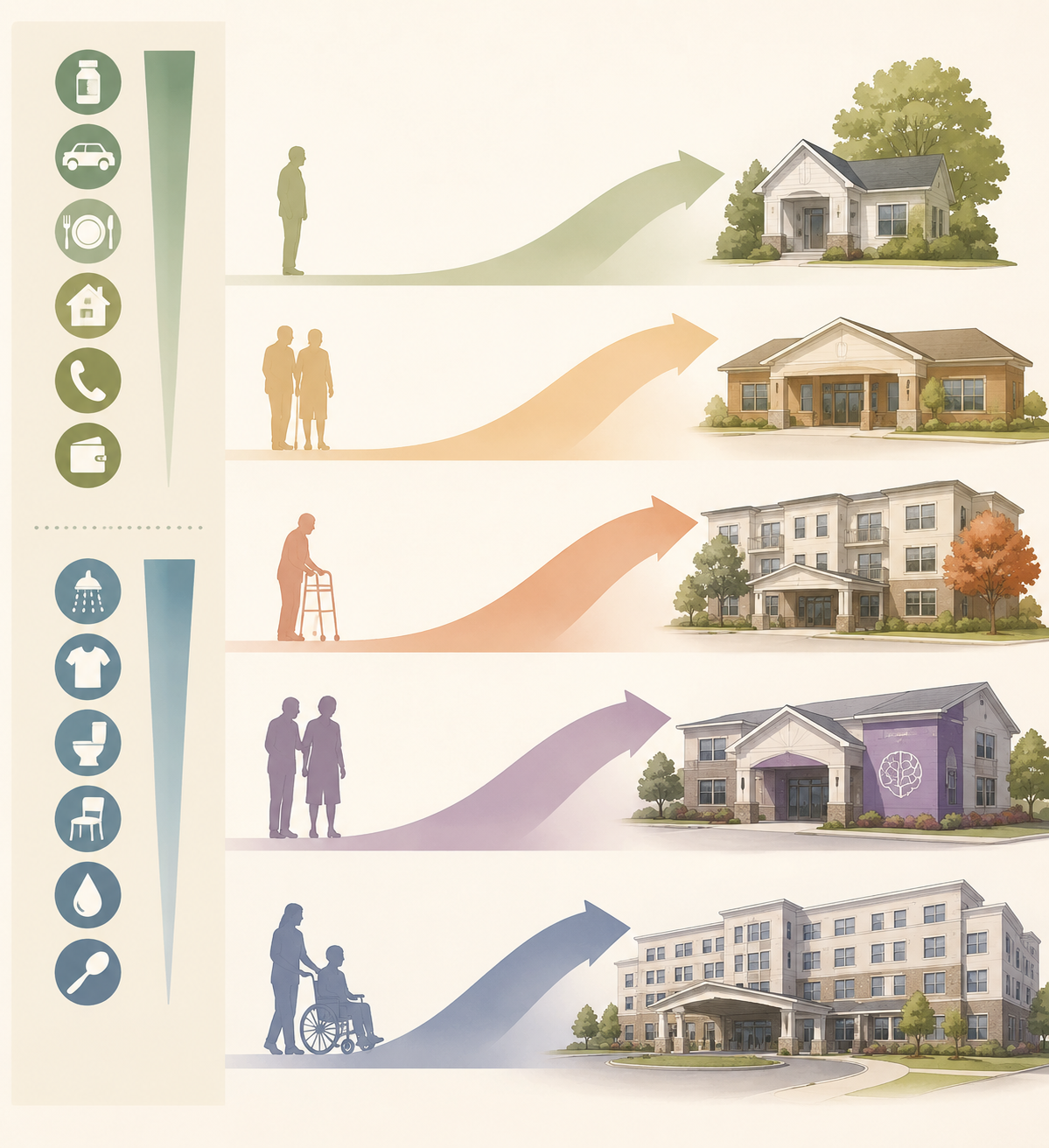
The shared language for that progression is ADLs and IADLs. ADLs, or activities of daily living, are the basic self-care tasks: bathing, dressing, toileting, transferring, continence, and feeding. IADLs, or instrumental activities of daily living, are the more complex tasks that let someone live independently: medication management, meal preparation, transportation, housekeeping, phone or communication use, and financial management. Doctors, senior living communities, insurers, and care planners all use some version of this framework when they evaluate care needs and costs.[1]
Start With What Is Already Failing
IADL losses often appear before a parent looks “disabled.” That is why families miss them. A person may still dress well, chat pleasantly, and insist nothing has changed while the practical machinery of independent life is quietly coming apart.
Medication management is usually one of the first pressure points. It is not enough that pills are present in the house or that a parent can name a medication. The question is whether the right dose is taken at the right time, day after day, without someone standing over the process. If the pillbox is wrong three days in a row, the care need has changed.
Transportation is another early marker. Giving up driving may look like a lifestyle change, but it can quickly become a care problem. Who gets the parent to appointments? Who notices when appointments are missed? Who handles the pharmacy, groceries, banking, and social connection that used to happen because the person could move through the community independently?
Meal preparation can be harder to read. Families may see snacks, takeout containers, or food in the refrigerator and assume eating is handled. The better evidence is weight change, spoiled food, burned pans, repeated skipped meals, or the same simple food eaten because sequencing a meal has become too much.
Housekeeping and finances tend to expose the same pattern. One late bill can be ordinary. A stack of unopened mail, duplicate payments, shutoff notices, missed insurance premiums, or unusual spending is different. Phone and communication problems matter too, especially when a parent can no longer reliably call for help, answer a care provider, or explain what happened.
No care path is perfectly orderly. Some families use adult day services for months. Some add home care until the budget or the caregiver gives out. Some move directly from home to memory care after wandering, hospitalization, or a frightening night. Still, the functional pattern is useful because it shows what each option is actually being asked to cover.
Functional reality
Care option that may fit
Where it often stops being enough
Mostly independent with mild IADL gaps
Family support, companion care, transportation help, medication setup
When reminders do not reliably produce the needed action
Needs supervision during the day but can return safely to a staffed or family home
Adult day services
When nights, wandering, toileting, or medication risk require continuous supervision
Needs help with meals, housekeeping, medication reminders, bathing, or dressing, but can use ordinary assisted living safely
Assisted living
When dementia behaviors exceed standard staffing, cueing, or safety capacity
Has dementia-related safety risks such as wandering, poor hazard awareness, serious medication errors, or unsafe nights
Memory care
When medical complexity, extensive transfers, wounds, or high nursing needs dominate
Needs round-the-clock nursing or rehabilitation-level medical care
Skilled nursing or nursing home care
When the primary need is no longer residential support but medical management
In-home care can work well when the missing pieces are specific and schedulable: help with meals, bathing, laundry, transportation, companionship, or medication reminders. The trouble starts when dementia does not respect the schedule. A four-hour shift cannot supervise a parent who leaves the house at 2 a.m. A weekday aide cannot solve weekend medication errors unless someone else owns the weekend system.
Adult day services can be a useful bridge when a person needs structure, meals, activities, and daytime observation. They can also give a spouse or adult child a predictable stretch of relief. But adult day care is not a substitute for safe evenings, overnight supervision, medication control, or hands-on help at home.
Assisted living enters when the parent needs a residential setting with help for daily tasks but does not yet require locked or dementia-specific supervision. It may cover meals, housekeeping, medication reminders, bathing help, dressing help, and routine checks. The word “assisted,” however, can hide a lot. Many assisted living communities are not built to manage repeated exit-seeking, unsafe cooking attempts, severe sundowning, or incontinence that requires frequent unscheduled care.
Skilled nursing belongs in the conversation when the care problem is medical as much as residential: rehabilitation after a hospitalization, complex wound care, extensive transfer assistance, serious mobility decline, or nursing needs that a memory care or assisted living community cannot safely meet.
When ADL Loss Changes the Weight of the Decision
ADL decline changes the care conversation because it turns supervision into hands-on responsibility. Bathing is often the first fight. A parent may insist they bathed, refuse the shower, forget the sequence, or become afraid of the bathroom. The result is not just odor or family embarrassment. It can mean skin problems, infections, falls, and a caregiver trying to physically coax someone through a task that used to be private.
Dressing loss may look mild until the same clothes are worn for days, winter clothing is chosen in heat, or soiled clothing is put back on because the person cannot judge what needs changing. Toileting and continence are heavier thresholds. Once accidents are frequent, care becomes urgent, repetitive, and time-sensitive. A setting that can remind someone to use the bathroom may not be able to clean, change, launder, and monitor them repeatedly throughout the day and night.
Transferring is another hard line. If a parent cannot safely move from bed to chair, chair to toilet, or chair to standing without help, the risk belongs to both the parent and the caregiver. One exhausted spouse trying to lift another person is not a care plan. Feeding decline usually comes later, but when it appears, families need to look closely at weight loss, choking risk, food refusal, and whether the person can stay seated and complete a meal.
These details matter because senior care placement is often decided less by the diagnosis than by the task list. “Early dementia” can still include a parent who cannot manage insulin, pay bills, or cook safely. “Moderate dementia” can include someone who is physically strong enough to leave the house but cognitively unable to find the way back.
The Memory Care Threshold
Memory care becomes necessary when ordinary help no longer keeps the person or caregiver safe. It is not simply assisted living with a dementia label. Memory care is designed for residents with Alzheimer’s disease or other dementias who need a more controlled environment, dementia-trained staff, structured routines, and security features that reduce the risk of unsafe exit-seeking.[2]
The first marker is wandering or elopement risk. A parent who walks around the house is not the same as a parent who leaves the house, enters traffic, goes out in unsafe weather, or cannot explain where they are. Families often wait for the second episode because the first one feels like an exception. From a safety standpoint, one true wandering event is enough to change the risk profile.
The second marker is loss of safety awareness. This includes the stove, smoking materials, traffic, strangers at the door, unsafe tools, spoiled food, or the inability to respond appropriately to an emergency. The parent may still sound reasonable in conversation. The question is whether judgment appears at the moment it is needed.
The third marker is medication error that requires supervision rather than reminders. A reminder assumes the person can understand the prompt, identify the correct medication, take the correct dose, and not repeat the dose later. When that chain fails, families are no longer arranging convenience. They are managing medical risk.
The fourth marker is incontinence beyond the capacity of standard assisted living. Occasional help is one thing. Frequent accidents, nighttime changes, resistance to hygiene, skin breakdown, or the need for repeated unscheduled assistance may require a staffing model that ordinary assisted living cannot provide reliably.
The fifth marker is caregiver safety. This includes exhaustion, fear, physical strain, aggression, unsafe nights, and the caregiver’s inability to leave the person alone long enough to shop, sleep, work, or recover. Caregiver burnout is sometimes discussed as an emotional issue, but in dementia care it is also a safety issue. A collapsing caregiver can no longer be the backup system.
Sundowning often sits across several of these markers. Late-day confusion, agitation, pacing, exit-seeking, or resistance to care can make a home arrangement look workable at noon and impossible by evening. The decision should be based on the hardest hours of the day, not the best visit.
For families trying to compare what they are seeing at home against a broader warning-sign list, 10 Signs It's Time for Memory Care can help separate ordinary forgetfulness from patterns that require a different level of supervision. If the parent is already in assisted living, the more specific question is covered in When to Move From Assisted Living to Memory Care.
Dementia Stage Helps, but Function Decides
Dementia stages can help families anticipate what may come next. The Alzheimer’s Association describes care needs as changing across early, middle, and late stages, with progression varying widely from person to person.[3] Stage language is useful, but it should not override the evidence in the house.
A parent in an earlier stage may still need more support if they live alone, manage risky medications, drive unsafely, or have no reliable local caregiver. Another parent with more obvious memory loss may remain stable longer because meals, transportation, medication administration, and supervision are already built into the day.
This is why a care notebook can be more useful than a family debate. Track missed medications, meals, falls, wandering attempts, hygiene changes, unpaid bills, nighttime events, and caregiver sleep. Bring that record to the physician, care manager, discharge planner, or senior living assessment. Vague concern invites vague reassurance. Dates and repeated breakdowns force a more serious conversation.
Families in the first month after a diagnosis or crisis can use The Adult Child Caregiver's First 30 Days to turn that evidence into immediate tasks instead of trying to solve the whole future at once.
What Care Costs Look Like Once Function Is Clear
Cost comparisons are useful only after the care need is named. Adult day services may be far less expensive than residential care, but they do not cover the night. Assisted living may cost less than memory care, but it may be the wrong purchase if the parent is already wandering. In-home care may feel less disruptive, but the hours add up quickly.
Care option
2026 national median or benchmark
What the number can hide
Adult day services
About $1,600 per month
Lower cost, but limited to scheduled hours and not a substitute for overnight safety
Assisted living
$6,200 per month, or $74,400 per year
May not include dementia supervision or higher hands-on care needs
Memory care
$7,645 per month
Typically carries a 20% to 30% premium over assisted living
In-home care
About $80,080 per year at 44 hours per week
Can become expensive when supervision must expand beyond scheduled shifts
Semi-private nursing home room
$9,581 per month, or $114,974 per year
Reflects nursing-level care, not simply more residential support
Private nursing home room
$10,798 per month, or $129,575 per year
Often driven by medical complexity and room type
U.S. News, citing CareScout data, reported those 2026 national medians and also noted that assisted living costs rose 5% from 2024 to 2025, while nursing home costs rose by about 1.5% to 3%.[4] These are directional figures, not local quotes. Geography can change the answer sharply, and families should price the actual county or metro area where care will be delivered.
The bigger mistake is comparing monthly prices without comparing coverage. Eight hours of home care may be enough for meals, bathing, errands, and companionship. It is not enough if the parent is unsafe during the other sixteen hours. An assisted living apartment may look affordable until the community adds care-level fees or says the parent now needs memory care. A memory care fee may look high until the family counts the private aides, unpaid leave, emergency calls, and caregiver health costs holding the home arrangement together.
What Medicare, Medicaid, VA Benefits, and Insurance Actually Change
Medicare is the payer families most often misunderstand. It does not pay for custodial memory care. Medicare may cover short-term skilled nursing or rehabilitation after a qualifying hospital stay, with coverage up to 100 days and cost sharing after day 20, but that is not the same as paying for long-term residential dementia care.[1]
Medicaid can help with long-term care for people who meet strict financial and functional eligibility rules. In many states, the asset limit is around $2,000, and Medicaid uses a five-year look-back period for asset transfers.[1] The exact benefits, waiver availability, and memory care coverage rules vary by state, so families need state-specific advice before spending down or moving money.
VA Aid and Attendance can help eligible veterans and surviving spouses pay for care. U.S. News reported 2026 monthly maximums of up to $2,424 for a single veteran and $2,874 for a married veteran.[4] Those amounts can matter, but they rarely cover the full cost of memory care by themselves.
Long-term care insurance depends on the policy, the benefit trigger, the elimination period, daily or monthly limits, and whether the diagnosis and ADL losses meet the contract terms. Amplify Life reported that 78% of long-term care insurance policies are purchased between ages 50 and 69, and that 47% of applicants age 70 and older are denied.[5] For families shopping after dementia symptoms are already present, traditional coverage may no longer be available.
Why Planning Often Skips Steps
The neat version of senior care moves from family help to home care, then assisted living, then memory care, then skilled nursing if medical needs increase. Real life often jumps. A parent falls and is discharged from the hospital with new transfer needs. A spouse hides the severity of nighttime wandering until they are exhausted. An assisted living community calls a care conference after repeated exit attempts. A daughter discovers the bills and the stove problem in the same weekend.
The broader long-term care numbers explain why these decisions are so common. Amplify Life reported that 70% of Americans who reach age 65 will eventually need some form of long-term care, and that more than 42% of long-term care residents have Alzheimer’s disease or related dementias.[5] Cognitive decline is not a side issue in senior care planning. It is one of the main reasons families have to move from informal help to supervised care.
U.S. News also cited CareScout CEO Samir Shah’s estimate that about 60% of assisted living residents eventually move to higher levels of care, with memory-related decline described as the most common driver.[4] That is an industry estimate rather than a peer-reviewed rate, but it matches what many families experience: assisted living can be a good fit for a time, and then dementia changes the job.
There is also evidence that memory care can change where people go next. A 2022 study published through PMC/NIH found that memory care reduced nursing home placement risk among assisted living residents with dementia.[6] That does not mean memory care prevents every nursing home move. It means dementia-specific residential care may help some residents remain outside nursing homes longer than they otherwise would.
When home is already unstable, planning has to become practical quickly. When Home Is No Longer Safe is the more appropriate next step for families who are past watchful waiting and need a crisis-to-plan structure.
How to Choose Without Pretending the Choice Is Easy
A workable decision starts with the current task failures, not with the most comforting label. Write down which IADLs are no longer reliable. Then write down which ADLs require cueing, setup, hands-on help, or total assistance. Add the dementia-specific risks: wandering, unsafe cooking, medication errors, sundowning, aggression, incontinence, falls, and whether the caregiver can sleep.
If the problems are limited, predictable, and schedulable, family support, home care, transportation help, or adult day services may be enough.
If the parent needs daily residential support but can still live safely with ordinary staffing, assisted living may fit.
If dementia creates unsafe wandering, poor hazard awareness, serious medication risk, unmanageable nights, or caregiver safety concerns, memory care should be evaluated.
If the main needs are medical, rehabilitation-based, or nursing-intensive, skilled nursing belongs in the discussion.
When evaluating a community, ask about the exact failure points you have observed. Do not ask only whether they “handle dementia.” Ask what happens when a resident tries to leave, refuses bathing, misses meals, becomes agitated at dusk, has repeated accidents, or needs medication administered rather than reminded. Ask what triggers a move-out notice or transfer to a higher level of care.
Families comparing facilities can use How to Choose a Senior Citizen Home for the site-visit and decision process. For dementia-specific stage matching, Dementia Care Options can help place the current situation in a longer disease course.
The right option is the least restrictive setting that can reliably meet the parent’s current ADL, IADL, and dementia safety needs. “Reliably” is the word that does the work. A plan that succeeds only when the parent has a good day, the caregiver is rested, the aide arrives on time, and nothing happens overnight is not yet a reliable plan.
Memory care becomes the necessary next step when ordinary supervision can no longer protect the person with dementia or the person trying to care for them.


Comments
Join the discussion with an anonymous comment.