Senior Care Options: A Complete Comparison Guide for Families Choosing the Right Level of Care
stage guideReviewed: 2026-06-19
Senior Care Options: A Complete Comparison Guide for Families Choosing the Right Level of Care
This guide helps adult children and family caregivers compare senior care options side-by-side — from in-home care and adult day care to assisted living, memory care, and skilled nursing. Learn how to match your loved one's current needs to the right care level using an ADL/IADL assessment, compare costs within the same care type, and avoid common decision-making pitfalls.
By Editorial Team
senior care options
assisted living
memory care
skilled nursing
in-home care
adult day care
ADLs
IADLs
care coordination
The Senior Care Spectrum: From Occasional Help to 24/7 Skilled Nursing
Senior care is not a single product you buy once. It is a spectrum of services that ranges from a few hours of weekly help with grocery shopping to round-the-clock skilled medical care. The mistake many families make is jumping straight to facility names — "Should we look at assisted living or a nursing home?" — before they understand where their loved one actually falls on this spectrum.
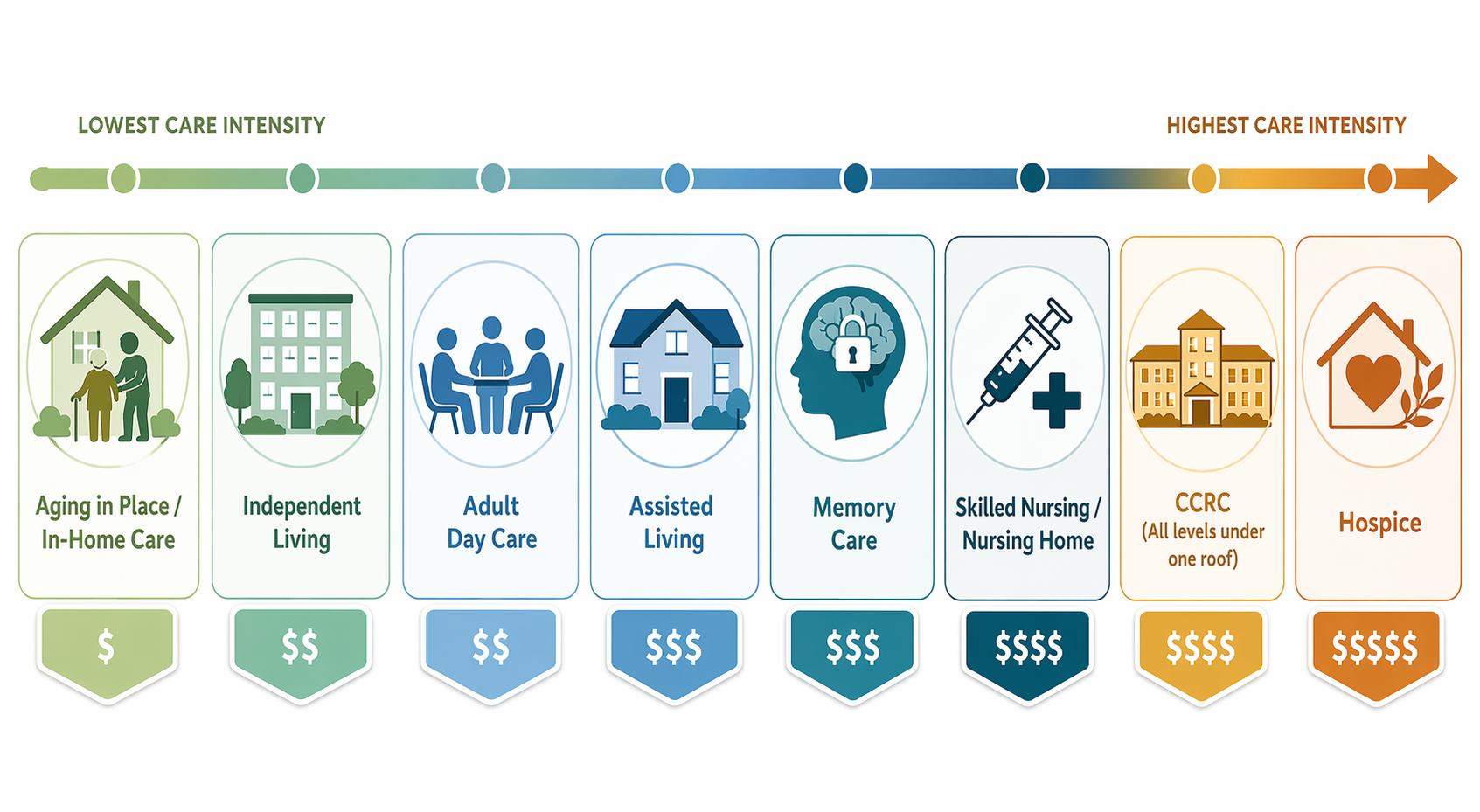
The goal is not to find the "best" option in absolute terms. It is to match the care level to the person's current functional needs and anticipated trajectory. Here is the landscape, arranged from least to most intensive:
In-home care (non-medical): A caregiver comes to the home for a set number of hours per week to help with bathing, dressing, meal preparation, light housekeeping, or companionship. Does not include skilled nursing.
Adult day care: A supervised, social, and sometimes therapeutic setting that operates during business hours. Ideal for older adults who cannot be left alone safely but whose primary caregiver works during the day.
Independent living: Age-restricted housing (apartments or cottages) with minimal or no built-in care services. Residents are generally able to manage their own activities of daily living (ADLs).
Assisted living: A residential setting that provides help with ADLs (bathing, dressing, medication management) but not 24/7 skilled nursing. Residents typically need moderate assistance.
Memory care: A specialized form of assisted living designed specifically for people with Alzheimer's disease or other dementias. Features secure environments, specially trained staff, and structured therapeutic programming.
Skilled nursing facility (nursing home): Provides 24/7 skilled nursing care, rehabilitation therapy, and medical monitoring for individuals with complex medical needs who cannot be cared for at home or in assisted living.
Continuing care retirement community (CCRC): A single campus that offers independent living, assisted living, and skilled nursing under one roof. Residents move between levels as their needs change.
Board and care homes (residential care homes): Small, home-like settings (typically 4–10 residents) that provide personal care and meals. Less institutional than assisted living but offer similar services.
Respite care: Short-term, temporary care (a few days to a few weeks) designed to give family caregivers a break. Can be provided in-home, in a facility, or through adult day care.
Hospice care: Comfort-focused care for individuals with a terminal illness (typically six months or less to live). Can be provided at home, in a hospice facility, or in a nursing home.
Each of these options serves a different point on the care continuum. The critical insight is that staying at home with full-time care is often the most expensive option — not the cheapest. According to U.S. News (April 2026, citing CareScout's 2025 Cost of Care Survey), a home health aide at $35/hour for 44 hours per week amounts to $80,080 per year. Expert Jacqui Clark states plainly: "Staying at home with care is the most expensive option. It's a big myth that it's cheaper to stay at home with care."
The Senior Care Spectrum: Matching Care Level to Need
Senior Care Options at a Glance: Side-by-Side Comparison
The table below summarizes each major care type across the dimensions that matter most for decision-making: who it serves, what services are included, the 2026 national median monthly cost, and key considerations. Cost figures are drawn from multiple sources (CareScout, Genworth, SeniorLiving.org, A Place for Mom) and represent national medians — your local costs may vary significantly.
2026 National Median Monthly Costs for Senior Care Options (sources: U.S. News/CareScout, SeniorLiving.org/Genworth, Senioridy, A Place for Mom)
Care Type
Who It Serves
Typical Services
2026 National Median Monthly Cost
Key Considerations
In-home care (non-medical)
Seniors who need help with ADLs/IADLs but want to remain at home
Less institutional than assisted living. Staff-to-resident ratios are often better. State licensing varies widely.
Respite care
Family caregivers who need a short-term break; seniors recovering from a hospital stay
Short-term personal care, meals, supervision (in-home or facility-based)
$350/day (U.S. News/CareScout 2025); $36.07/hour at home (SeniorLiving.org/Genworth 2026)
Essential for preventing caregiver burnout. Some states offer respite vouchers. Medicare may cover short-term skilled respite.
Hospice care
Individuals with a terminal illness (typically 6 months or less to live)
Pain management, symptom control, emotional and spiritual support, caregiver support
Varies widely; covered by Medicare Hospice Benefit, Medicaid, and most private insurance
Focus is on comfort, not cure. Can be provided at home, in a hospice facility, or in a nursing home. No copayment under Medicare Part A.
How to Determine the Right Care Level: Using ADLs and IADLs
Before you can compare costs or tour facilities, you need to determine what level of care your loved one actually needs. The most reliable framework for this is the ADL (Activities of Daily Living) and IADL (Instrumental Activities of Daily Living) assessment. These are the standard measures that healthcare professionals, state regulators, and facility care plans use to determine care needs.
What Are ADLs and IADLs?
ADLs are the basic self-care tasks that a person must be able to perform to live independently. IADLs are more complex tasks that require higher-level cognitive and organizational skills. A person typically loses IADL abilities first, then ADLs as function declines.
ADL and IADL Assessment Checklist
Category
Activity
What to Assess
ADL
Bathing
Can they bathe independently, or do they need help getting in/out of the tub or washing hard-to-reach areas?
ADL
Dressing
Can they select appropriate clothing and put it on without assistance? Do they struggle with buttons, zippers, or shoes?
ADL
Eating
Can they feed themselves? Do they need help cutting food or have difficulty swallowing?
ADL
Transferring
Can they get in and out of bed, a chair, or a wheelchair without help? Do they use a walker or cane?
ADL
Toileting
Can they get to and from the toilet, clean themselves, and manage incontinence products independently?
ADL
Continence
Do they have bladder or bowel control? Do they need reminders or assistance with incontinence management?
IADL
Medication management
Can they take the correct dose at the correct time? Do they need reminders or pill organization?
IADL
Meal preparation
Can they plan and cook a balanced meal safely? Do they forget to eat or leave the stove on?
IADL
Housekeeping
Can they maintain a reasonably clean and safe living environment? Is the home cluttered or dirty?
IADL
Transportation
Can they drive safely? Can they use public transportation or arrange rides?
IADL
Money management
Can they pay bills, balance a checkbook, and avoid financial scams? Are there unpaid bills or unusual spending?
IADL
Communication
Can they use the phone, respond to messages, and manage appointments?
How ADL/IADL Dependencies Map to Care Levels
The number and type of dependencies provide a rough but reliable guide to the appropriate care level:
0 ADL dependencies + 1–2 IADL dependencies: In-home care (a few hours per week) or adult day care. The person needs help with complex tasks like medication management or transportation but can manage basic self-care.
0–1 ADL dependencies + 3+ IADL dependencies: Assisted living or board and care home. The person needs help with daily living tasks but does not require 24/7 skilled nursing.
2–3 ADL dependencies (especially bathing, dressing, and transferring): Assisted living with a higher level of personal care, or memory care if dementia is present. The person needs hands-on assistance with multiple basic tasks.
4+ ADL dependencies or complex medical needs (e.g., wound care, tube feeding, ventilator): Skilled nursing facility. The person requires 24/7 nursing care that cannot be provided in a residential setting.
Dementia diagnosis with wandering, aggression, or safety concerns: Memory care, regardless of ADL count. The specialized environment and staff training are necessary for safety.
Mapping ADL/IADL Dependencies to Care Levels
The Three-Step Decision Framework: Compare Within the Same Care Level
Once you know the care level your loved one needs, the actual decision-making becomes much simpler. The most common mistake families make is comparing options across different care levels — for example, asking "Is assisted living cheaper than a nursing home?" when the person clearly needs skilled nursing. That comparison is meaningless because the two options serve fundamentally different needs.
Here is the three-step framework:
Step 1: Lock the Care Level First
Use the ADL/IADL assessment above to determine the appropriate care level. Write it down. Do not move to Step 2 until you are confident about this. If you are unsure, consult with the person's primary care physician, a geriatric care manager, or a hospital discharge planner.
Step 2: Compare Options Within That Specific Care Level
Now that you know the care level, compare providers within that level. For assisted living, compare multiple assisted living communities. For memory care, compare memory care communities. For in-home care, compare home care agencies. Do not compare across levels — the cost, services, and regulatory requirements are fundamentally different.
When comparing within a level, evaluate:
Staff-to-resident ratios and staff turnover rates
Included services vs. add-on services (what is included in the base monthly fee?)
Care assessment process (how do they determine and update the care plan?)
Safety and security features (emergency call systems, secure exits, lighting)
Activities and programming (is it engaging and appropriate for the person's cognitive level?)
Meal quality and dietary accommodations
Inspection history and any past violations
Step 3: Verify with Official Sources
Before making a final decision, verify your shortlisted options using independent, authoritative sources:
Medicare's Care Compare tool (medicare.gov/care-compare) — provides quality ratings and inspection results for nursing homes, home health agencies, and hospices.
State health department inspection reports — available for nursing homes and, in many states, for assisted living and memory care communities.
The Joint Commission's Quality Check (qualitycheck.org) — accreditation status for healthcare organizations.
National Institute on Aging (NIA) checklists — provides step-by-step guidance for choosing a nursing home or other long-term care facility.
The Three-Step Decision Framework
2026 Cost Benchmarks: What Each Care Type Really Costs
Understanding the true cost of each care type is essential for financial planning. The figures below represent 2026 national median costs from multiple sources. Remember that actual costs vary by geographic region, level of care needed, and specific facility.
2026 National Median Monthly Costs for Senior Care Options (multiple sources)
Care Type
2026 National Median Monthly Cost
Source
Key Note
Home health aide (44 hrs/week)
$6,677
SeniorLiving.org/Genworth 2026
Full-time (44 hrs/week) is often the most expensive option. 24/7 live-in care can exceed $10,000–$15,000/month.
Homemaker services (44 hrs/week)
$6,878
SeniorLiving.org/Genworth 2026
Slightly more than home health aide due to different survey methodology.
Adult day care
$2,058
U.S. News/CareScout 2025
Cost-effective alternative to full-time care. $80–$150 per day.
Independent living
$3,523
U.S. News/CareScout 2025
No built-in care services. Costs vary significantly by location and amenities.
Assisted living
$6,200–$6,259
U.S. News/CareScout 2025; SeniorLiving.org/Genworth 2026
Median cost surged 10% in 2024 to $70,800 annually (New LifeStyles).
Memory care
$6,690–$8,019
A Place for Mom 2026; SeniorLiving.org 2026
20–30% more than standard assisted living. State medians range from $5,538 (SD) to $14,399 (HI).
Skilled nursing (semi-private room)
$9,581–$9,842
U.S. News/CareScout 2025; SeniorLiving.org/Genworth 2026
Annual cost exceeds $114,000–$118,000.
Skilled nursing (private room)
$10,798–$11,294
U.S. News/CareScout 2025; SeniorLiving.org/Genworth 2026
Annual cost now exceeds $127,750 (New LifeStyles).
Board and care home (private room)
$7,300
U.S. News/CareScout 2025
Less institutional than assisted living. State licensing varies.
High upfront cost. Financial stability of the CCRC is critical.
Respite care
$350/day (facility); $36.07/hour (at home)
U.S. News/CareScout 2025; SeniorLiving.org/Genworth 2026
Short-term. Essential for caregiver burnout prevention.
The Tour Checklist: Questions to Ask at Every Facility or Agency
Whether you are touring an assisted living community, a memory care unit, or a board and care home, the same core questions apply. Use this checklist as a printable reference tool during your visits.
Staffing and Care
What is the staff-to-resident ratio during the day? Overnight?
What is the annual staff turnover rate? How long has the average caregiver been employed here?
What training do staff members receive? Is there specialized training for dementia care, medication management, or fall prevention?
How is the care assessment conducted? How often is it updated? Who participates?
What is the process for handling a medical emergency? Is a nurse on-site 24/7?
Services and Costs
What is included in the base monthly fee? What services are charged as add-ons?
How are rate increases handled? What has been the average annual increase over the past 3 years?
Is there a community fee or entrance fee? Is it refundable?
What happens if the resident's care needs increase? Is there a separate memory care or skilled nursing unit on-site?
Safety and Environment
Is the facility secure? Are there locked entrances, keypad entries, or wander management systems?
Are there grab bars, non-slip flooring, and adequate lighting in hallways and bathrooms?
What is the emergency evacuation plan? How are residents with mobility challenges evacuated?
What is the most recent state inspection rating? Have there been any violations in the past 3 years?
Activities and Quality of Life
What is the daily activity schedule? Are activities tailored to different cognitive and physical ability levels?
Can residents personalize their rooms? Are pets allowed?
What is the meal service like? Can residents choose from a menu? Are dietary restrictions accommodated?
How does the facility support family involvement? Are there family councils or regular family meetings?
How to Pay for Senior Care: Medicare, Medicaid, VA Benefits, and More
Understanding how to pay for senior care is often the most confusing part of the decision. The key distinction to remember is that Medicare does not cover long-term custodial care — meaning it will not pay for assisted living, memory care, or nursing home room and board for ongoing care. Here is a summary of the major payment sources:
Summary of Major Payment Sources for Senior Care
Payment Source
What It Covers
What It Does NOT Cover
Key Details
Medicare (Part A)
Up to 100 days of skilled nursing care after a qualifying 3-day hospital stay; hospice care; some home health care
Long-term custodial care in a nursing home, assisted living, or memory care; room and board in senior living
Covers short-term rehabilitation only. After day 20, a daily copayment applies. Must be in a Medicare-certified facility.
Medicare (Part B)
Doctor visits, outpatient care, some home health services, durable medical equipment
Long-term care, personal care, room and board
Covers medically necessary services, not custodial care.
Medicare Advantage (Part C)
Same as Part A and B; some plans offer additional benefits like adult day care or meal delivery
Long-term custodial care; varies by plan
Coverage varies significantly by plan and state. Check your plan's Summary of Benefits.
Medicaid
Long-term nursing home care for low-income individuals; some states cover assisted living and home care through waivers
Room and board in assisted living or memory care (in most states); varies by state
Primary payer for long-term nursing home residents. Requires spend-down of assets. Subject to a 5-year look-back period. Rules vary by state.
VA Aid and Attendance
Up to $2,424/month for single veterans; $2,874/month for married veterans; $1,558/month for surviving spouses (U.S. News/CareScout 2025)
Does not cover all costs; must be used for care-related expenses
Available to veterans and surviving spouses who need help with ADLs. Requires a VA medical exam. Can be used for in-home care, assisted living, or nursing home.
Long-term care insurance
A range of services including home care, assisted living, memory care, and nursing home care
Pre-existing conditions may be excluded; premiums can increase
Best purchased before care is needed (typically in your 50s or early 60s). Policies vary widely in coverage and exclusions.
Private pay
Any care type; no restrictions
Depletes savings quickly
The fastest way to pay for care. Median annual cost of a private nursing home room now exceeds $127,750 (New LifeStyles 2026).
When to Start the Conversation: Avoiding Crisis-Driven Decisions
The single best thing you can do for your family is to start the conversation about senior care options before a crisis occurs. Research shows that crisis-driven decisions — made after a fall, a hospitalization, or a dementia diagnosis — lead to worse outcomes, higher costs, and more stress for everyone involved.
Here is why early planning matters:
More options available: Many facilities have waitlists, especially for memory care units. Starting early gives you access to a wider range of choices.
Better financial outcomes: You have time to explore Medicaid planning, VA benefits, and long-term care insurance before assets are depleted.
Lower emotional stress: Decisions made in a panic are rarely the best decisions. Early planning allows for thoughtful, collaborative family discussions.
The person's voice is heard: When you start early, your loved one can participate in the decision-making process. In a crisis, decisions are often made for them, not with them.
How to Start the Conversation
Initiating a conversation about senior care with a parent or spouse is often the hardest part. Here are practical tips:
Frame it as planning, not taking over: "I want to make sure we have a plan in place so that if something happens, we're not scrambling. Can we talk about what you'd want?"
Focus on values and preferences first: Ask about what matters most — staying at home, being near family, having a private room, access to outdoor space.
Use a neutral third party: A geriatric care manager, social worker, or the person's primary care physician can help facilitate the conversation.
Start small: Begin with a single topic, like home safety or medication management, rather than trying to decide on a facility in one conversation.
Acknowledge the emotional weight: "I know this is hard to talk about. It's hard for me too. But I want to make sure we make decisions together, not in a rush."



Comments
Join the discussion with an anonymous comment.